Intradural disc herniations (IDH) are very rarely reported in the literature with an estimated incidence ranging between 0.04-1.5%, affecting males more than females with an onset between 50-60 years of age [1,2]. IDH is defined as fragmented disc material that breaks through the annulus, posterior longitudinal ligament (PLL), and dura migrating into the thecal sac. The exact etiology is unknown, but a few theories have been proposed, including fibrosis or adhesions of the dura to the annulus, prior history of spinal surgery, congenital narrowing, advanced degenerative disc disease with resulting chronic inflammation leading to erosion and dural thinning, congenital dura thinness or fusion between the dura and posterior ligaments [3-7].
The majority of cases reported in the literature suggest a clinical picture of acute-on-chronic lower back pain (LBP) with bilateral lower extremity pain, motor and/or sensory findings, often accompanied by symptoms of cauda equina syndrome (CES). Magnetic resonance imaging (MRI) is required to define the location of the disc pre-operatively, but the absolute diagnostic confirmation is made intraoperatively [5-7]. Treatment of IDH is often surgical, and there is a paucity of literature regarding interventional pain management outcomes, prognosis, and follow-up due to the rarity of this condition. We report a unique case presentation of IDH at the L3-4 level, initially managed with lumbar epidural steroid injection (LESI) due to patient preference to avoid surgery, but ultimately requiring surgical intervention due to progressive neurologic deficits. The patient provided written consent for the publication of this report.
CASE REPORT
A 54-year-old male with body mass index of 32 presented with a one-month history of acute-on-chronic LBP following heavy lifting during a recent move. The pain was experienced constantly, characterized as sharp, stabbing, and shooting, and radiated into the right buttock, lateral hip, and anterior thigh. He had associated right lower extremity numbness and tingling, in addition to weakness affecting the gluteal and quadriceps muscles. Pain was worse with lying supine and improved with sitting. He reported new onset difficulties with ambulation, including navigating stairs, transfers, and activities of daily living. Visual analog pain score was reported at 10/10. He denied symptoms of saddle anesthesia, bowel or bladder dysfunction and other CES-like symptoms. He tried over-the-counter analgesics, opioids, muscle relaxants, gabapentinoids and therapeutic exercises without improvement. Of note, he reported that these symptoms were significantly different from his intermittent axial, non-radicular LBP symptoms, which typically resolved spontaneously in 2-3 weeks with over-the-counter analgesics and adherence to his home-exercise program.
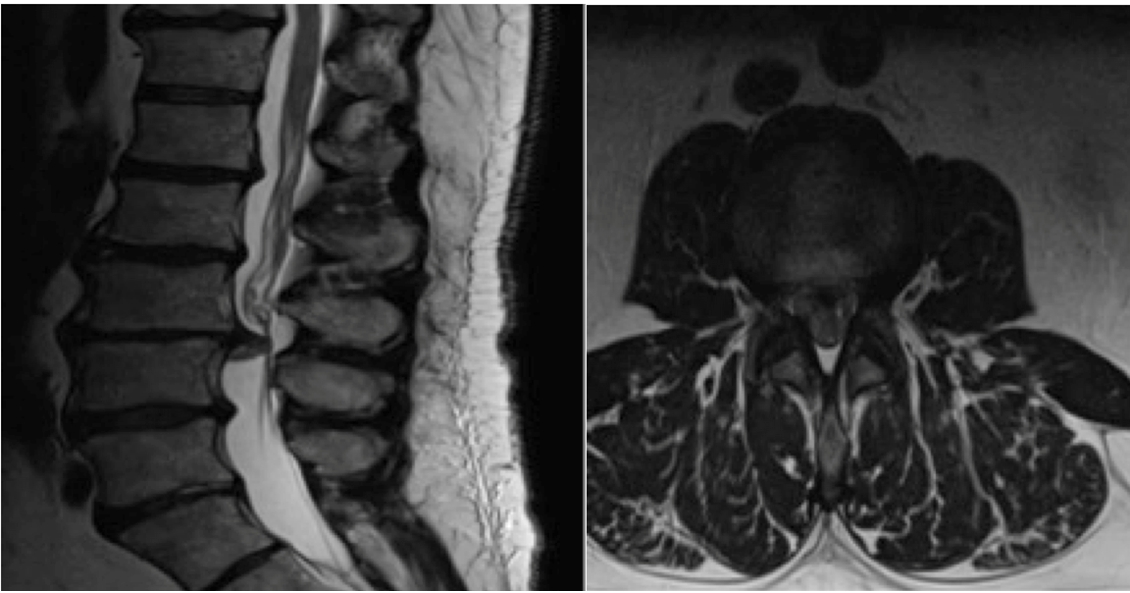
The patient was evaluated by a neurosurgeon and an interventional pain medicine physician. Physical exam revealed 5/5 strength on manual muscle testing of the bilateral lower extremities, except for 4/5 strength in the right quadriceps and hamstrings muscles. Sensation was intact to light touch in all dermatomes throughout the bilateral lower extremities. Perineal sensation was intact. Right-sided straight-leg raise was positive eliciting increased low back pain with aggravation of pain and tingling down the right leg, including the gluteal region and anterior thigh. Right lower extremity deep tendon reflexes (DTRs) were hypoactive compared to the contralateral side. Babinski's sign was negative. MRI of the lumbar spine revealed high-grade central canal stenosis due to intradural disc herniation completely effacing the subarachnoid space and causing bilateral nerve root compression at the L3-4 level (Figs. 1, 2). The case was discussed among the neurosurgeon, pain physician and patient/family, and the decision was made to pursue a LESI as the patient declined surgery at this time, since he was leaving the city for an out-of-state job. The first LESI was performed roughly 6-weeks post injury. Due to nerve root redundancy above the level of the herniation (L3-4) and intolerance to injection at the L3-4 level due to pain, the epidural space at the L2-3 level was targeted via interlaminar approach under fluoroscopic guidance with notable cranial and caudal contrast spread (Fig. 3). A standardized solution of 1% lidocaine anesthetic and 80 mg of methylprednisolone acetate was injected. There were no procedural complications. At one-week follow-up post injection, the patient reported minimal pain relief, and the decision was made to proceed with a second LESI. Two weeks later, the patient underwent the second LESI by right-sided interlaminar approach at the same L2-3 level without complication. He reported approximately 40% overall improvement with reduction in pain, improved mobility, and increased ability to participate in daily activities and work duties. However, there was no recovery in motor weakness or DTRs at either post-injection follow-up visit.
At three-month follow-up post injury, the patient reported worsening and debilitating LBP characterized as sharp, electrical shock-like sensations involving the back and legs. Symptoms progressed from unilateral right-sided radiculopathy to bilateral lower extremity tingling and intermittent numbness. He reported that he had done ŌĆ£more than usualŌĆØ at work, particularly, he noted having ambulated 14,000 steps the day prior to pain exacerbation. He endorsed associated lumbar muscle spasms with impaired ability to stand or walk for more than five minutes. He reported significant fear-avoidance behavior and inability to find comfortable positions. He tried meloxicam, gabapentinoids and opioid analgesics, as well as physical therapy without improvement. The patient reconsulted with the neurosurgeon and the pain physician four months after initial injury. His physical examination was unchanged from prior visits and an updated lumbar spine MRI (Fig. 4) was obtained reconfirming the intradural location of the disc herniation without significantly increased mass effect on the nerve roots within the thecal sac. Based upon the progressive nature of the patientŌĆÖs symptoms, the decision was made to proceed with surgical intervention.
In this case, the patient underwent an L3-L4 laminectomy and intradural resection of the disc herniation (Fig. 5). The ventral dural rent was identified and noted to be adherent to the annulus of the L3 disc space. Following complete resection of the intradural disc herniation, the dural was closed primarily. The dural repair was tested with intraoperative Valsalva to 30 mm water with no evidence of cerebrospinal fluid (CSF) leak. The dural repair was reinforced with Tissel┬« and the remainder of the incision was closed in anatomical layers. Intraoperative motor evoked potential monitoring was performed throughout the course of the case, and there was no change between the preoperative and intraoperative recordings. The patient tolerated the procedure well, was monitored for cerebral spinal fluid leak post-operatively, and ultimately discharged on post-operative day 4 to acute inpatient rehabilitation. At the 6-week postoperative visit, the patientŌĆÖs symptoms had resolved, his neurologic exam had normalized, and he was able to return to full employment without restriction. At five month follow-up, his Oswestry Disability Score was 8/50 (16%), a 79% decreased from the pre-surgical score of 39/50 points (78%) of complete disability.
DISCUSSION
The first reported case of IDH was in 1942, and since other cases have been reported [1-4,6,8,9], yet it remains a very rare cause of lower extremity radiculopathy and CES [1-4, 7-9]. Most IDH are found in the lumbar spine (95%) with the L4-5 level being the most commonly affected (55%) followed by the L3-4 level (16%) and then the L5-S1 level (10%) [2,6]. IDH has a 4:1 male to female ratio with an average age of onset of 50-60 years [1-4,5-7].
The pathogenesis for IDH remains uncertain. Several factors are thought to be responsible for this atypical herniation, including narrowing of the spinal canal due to congenital or iatrogenic causes, adhesions between the annulus fibrosus, PLL, and dura, and dura fragility [1-4]. Adhesion formation is thought to be the most important factor [2,6-7]. In normal conditions, the PLL and the dura are loosely attached. However, in the setting of prior spinal surgery, chronic disc herniation and/or traumatic forces dense adhesions may form, predisposing the area to IDH [1-4,6-8]. These adhesions, attaching the dural sac to the anterior wall of the central canal, may pull extruded disc material into the dural space [1,7]. An anatomical investigation by Yildizhan et al. [7] demonstrated that the firmest attachment of the ventral dura to the PLL was at the L4-5 level, which coincides with prior prevalence reports [1-4,6,8].
There is no difference in clinical signs between IDH and extradural disc herniations [5,8-9]. However, most IDH cases, as reported in the literature, suggest a similar clinical presentation of acute-on-chronic LBP with associated bilateral lower extremity symptoms and higher incidence of CES. In fact, CES has been reported in up to 30% of IDH cases in comparison to 0.5-1% in other disc herniations [5,8]. In contrast to most cases currently reported in the literature, our case reports a rare unique clinical presentation without CES, without previous surgical history and with initial unilateral lumbosacral radiculopathy that over several months progressed to bilateral radicular symptoms, with IDH at the L3-4 level, only present in 16% of cases.
IDH remains a challenge to diagnose. Mut et al. [10] proposed a classification system for IDH: Type A: herniation of disc into the dural sac and Type B: herniation of disc into dural sheath in the preganglionic region of the nerve root (also named intraradicular disc herniation). Historically, IDH has been diagnosed intraoperatively. This is in large part due to its rarity and the propensity to confuse the pathology with other space occupying lesions in the spinal canal, such as meningiomas, metastases, cysts, etc [2,5-7].
Neuroradiology perspective
In the present case, the imaging appearance was adequate to confirm the diagnosis. In the literature, several MRI signs that are reported to suggest IDH include a "Y-sign" in the ventral dura in which the disc material splits the ventral dura and arachnoid mater on T2-weighted sagittal images, a "crumble disc sign" in which there is discontinuity of the PLL and anterior thecal sac on T2-weighted sagittal images, and a ŌĆ£hawk-beak signŌĆØ in which a beak shaped lesion compresses the dural sac on T2-weighted axial images [6,11-15]. If MRI cannot be performed, myelography can show the presence of soft tissue compressing the thecal sac or filling the thecal sac, as in the case of IDH [5,6,13]. In addition to being used for pre-operative planning, it can be used to characterize the degree of CSF block at the suspected level [5,6,11-13]. On the axial and sagittal MRI pictures (Fig. 4), the herniated disc was seen to penetrate the posterior longitudinal ligament and dura, with disc material and blood filling the thecal sac, as there are no intrathecal boundaries to expansion. The disc had marginal enhancement, typical of chronic herniation with surface granulation. The obvious extension from the disc space and marginal enhancement excluded entities such as tumor or infection [14]. There was no mass effect on the dura/ thecal sac, as is seen in typical herniations, as the bulk of the disc entered and filled the thecal sac.
The present case fits the typical demographic profile for IDH in the setting of previous disc herniation but is rare in that the IDH occurred at L3-4 level, reported in 16% of cases, and resulted in unilateral radiculopathy without CES [2,6]. Unilateral radiculopathy, the absence of CES, functional ambulatory status and no prior lumbar spine surgical history, such as in our case, have rarely been reported in cases of IDH [1-4,6-8,14,15]. Unilateral radiculopathy without CES are considered good prognostic indicators for pain and motor recovery, in contrast to the presence of previous disc herniations, history of spinal surgery, chronic symptoms and CES [5-8].
Neurosurgery perspective
Early surgical intervention has generally been considered the treatment of choice for IDH to prevent further neurologic decline [2,7-9]. To our knowledge, no case report exists on successful conservative treatment of IDH. The current case is rare not only in presentation, but also in management as this patient was initially treated conservatively with satisfactory pain relief and improved function for at least 4 months, prior to re-injury and progression of the IDH. It is unclear whether early surgical management of IDH in individuals with minimal neurologic deficits is superior to initial conservative management with delayed surgery. Nevertheless, conservative management with spinal injections may improve pain control and function temporarily pre-operatively. Definitive treatment of IDH is surgical, which should preferably be performed with a microsurgical approach with a paramedian or median dural incision for better visualization of the hernia and to avoid damage to spinal roots [2,7,12].
IDH is a rare and challenging diagnosis, as demonstrated by a limited number of case reports and imaging similarities to other spinal cord pathologies. While the pathogenesis of IDH remains uncertain, it appears likely that adhesion formation between the annulus fibrosus, PLL, and dura from prior spinal surgery, disc herniation, or trauma predispose patients to developing this atypical herniation. Diagnostic evaluation should include an MRI pre-operatively and evidence of a large central disc herniation. Some studies report that findings such as the "Y-sign," "crumble disc sign," and/or ŌĆ£hawk-beak signŌĆØ should raise suspicion for IDH. Confirmatory diagnosis is made intraoperatively, and definitive management remains surgical; however, patients with minimal neurologic deficits may initially be managed non-surgically with spinal injections to improve pain control, restore function and increase early mobilization during the preoperative phase.