Long thoracic nerve (LTN) neuropathy occasionally occurs in young people involved in various sports [1]. The LTN arises from the cervical roots (C5-C7) and innervates the serratus anterior (SA) muscle [2]. Scapular winging is the landmark manifestation of LTN neuropathy and may develop after an accidental injury [3]. However, LTN neuropathy can also occur without scapular winging and specific magnetic resonance imaging (MRI) findings [4]. Herein, we report a case of an 18-year-old male with LTN neuropathy successfully treated with an SA plane block and ultrasound (US)-guided hydrodissection.
CASE REPORT
Written informed consent for the procedure and publication of this report was obtained from the patient. An 18-year-old man with a height of 173 cm and weight of 50 kg was admitted to our hospital for the management of right-sided lateral chest pain. A more detailed history revealed that the pain originated 7 months prior when the patient performed repetitive push-ups. The patient was treated with analgesic medication, trigger point injection, and physical therapy for approximately 4 weeks in the rehabilitation department but was referred to our pain clinic because his symptoms did not improve. Blood test results (complete blood cell count, erythrocyte sedimentation rate, and C-reactive protein), chest radiography, and electrocardiogram (ECG) findings were normal. MRI of the right shoulder revealed no abnormality. The patient complained of pain in the distal part of the right shoulder and the right lateral side of the chest. Additionally, the patient complained of weakness in the right upper arm. On physical examination, there was a tender point in the pectoralis muscle area at the fifth rib and mid-axillary line. The symptom was provoked when the patient tilted his head away from his right arm and raised his right arm overhead. Furthermore, right-sided shoulder flexion (90˚) and abduction (120˚) were reduced compared to left-sided shoulder flexion (160˚) and abduction (180˚). Other ranges of shoulder motion and motor function testing were normal, and a winged scapula was not observed on the right side. The patient’s pain score on a visual analog scale (VAS; 0: no pain, 10: maximal pain) was 6. We performed a trigger point injection on the tender point in the right chest. However, the patient showed improvement in symptoms only 2 days after the injection. We then performed electromyelography (EMG). The EMG findings suggested LTN neuropathy in the right upper chest, which supported the findings of the physical examination. We suspected an injury of the LTN.
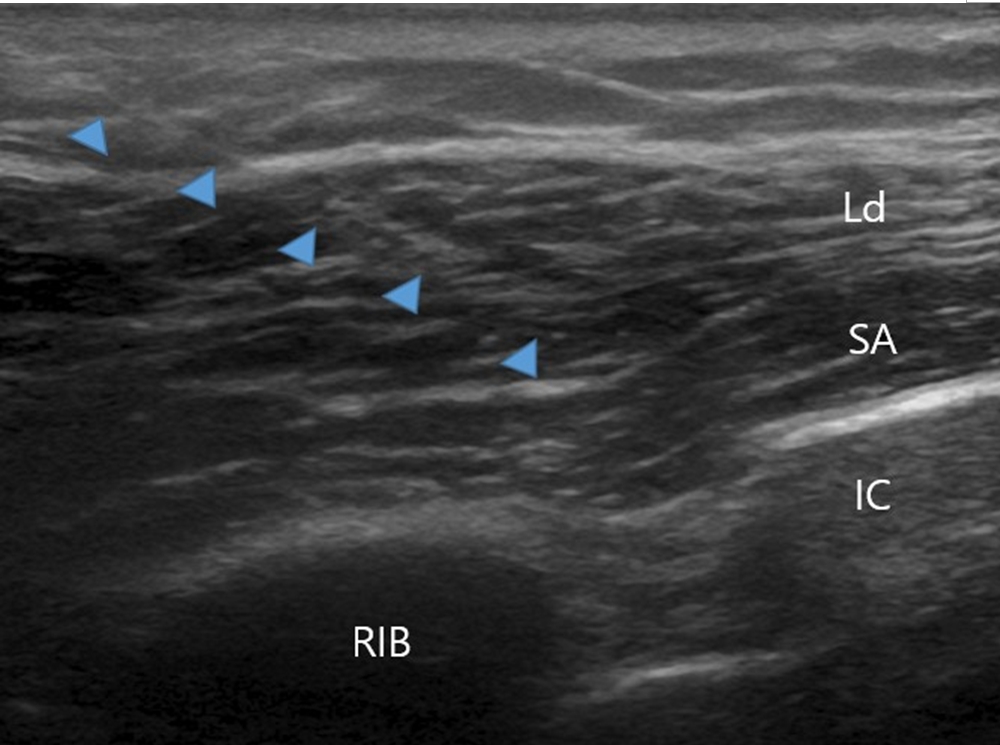
Since the LTN usually innervates a single muscle, the SA, we planned an SA plane block with US-guided hydrodissection. We explained the procedure and its benefits to the patient. After positioning the patient in the lateral decubitus position and ensuring a sterile operative field, we placed the linear probe (10-12 Hz) on the sagittal plane view for US scanning. Under real-time US guidance, we performed an SA plane block with hydrodissection. We selected the tender point above the fifth rib at the mid-axillary line as the needle insertion site. The needle was introduced in-plane from supero-anterior to postero-inferior. The needle tip was placed above the SA muscle. After identifying the fifth rib on the mid-axillary line, we were able to locate the SA, latissimus dorsi, and intercostal muscles on sagittal plane views. We placed a 25-G, 50-mm needle in the plane between the SA and latissimus muscle (Fig. 1). We injected 20 ml of bupivacaine 0.125% with triamcinolone 20 mg above the SA muscle, following a 1 ml test dose. The patient tolerated the procedure well with virtually no discomfort. We closely observed the patient’s peripheral oxygen saturation, ECG, and blood pressure for 30 min following the block. After 30 min, his VAS score decreased to 3. We repeated the SA plane block after 7 days, and his VAS score decreased to 2. The patient was reviewed after 1 week and 1, 2, and 3 months later. The patient had almost complete pain relief, with VAS pain scores of 0 or 1 during this period. In addition, the full range of shoulder motion returned without any functional limitations.
DISCUSSION
The LTN mainly arises from the C5-C7 nerve roots and sometimes from the C4 and C8 nerve roots [2,5]. The first two nerve roots, C5 and C6, form a superior trunk on the middle scalene muscle and join C7 to form the inferior trunk, which travels dorsally to the brachial plexus and the anterolateral portion of the chest wall. The LTN gradually travels toward the mid-axillary line beside the lateral thoracic artery [6]. Furthermore, the LTN divides into several branches to innervate the SA muscle, which makes clear visualization of the distal LTN more challenging. The LTN travels from the neck to the truncal region and is susceptible to direct trauma because of its long course and superficial location. LTN entrapment can occur between the middle and posterior scalene muscles, the first rib, the clavicle and the second rib, the second rib and the coracoid (under the pectoralis minor muscle), the inferior angle of the scapula, or an inflamed bursa along the course of LTN [6]. In this case, the tender point exited the pectoralis muscle at the fourth or fifth rib and mid-axillary line in the travel path of the nerve. Therefore, we selected the tender point as the injection site.
The LTN innervates the SA muscle, which originates from the first to ninth rib and inserts onto the superior angle, vertebral border, and inferior angle of the scapula [2]. The SA muscle plays an important role in shoulder function. It stabilizes the shoulder during arm elevation by fixing the scapula and allowing for scapular upward rotation [4]. In this case, the patient demonstrated limitations in flexion (90˚) and abduction (120˚) of the right shoulder. After the SA plane block with hydrodissection, his right shoulder’s flexion and abduction were restored to normal ranges, and his pain reduced.
There are several causes of LTN palsy, which can be traumatic or non-traumatic; the most common injury to the LTN is either trauma or sports-related [6]. Most traumatic injuries are caused by blunt trauma, such as sudden compression or twisting of the shoulder, which is usually due to nerve traction. Athletic postures such as the athlete’s head rotating away from the arm, raising the arm, throwing a ball, and spiking or serving a volleyball may cause injury [6,7]. Non-traumatic injuries include viral illness (such as poliomyelitis), allergic drug reaction, drug overdose, toxic exposure, muscular dystrophy, facioscapulohumeral muscular dystrophy, C7 radiculopathy, and aortic coarctation [1,6]. Considering the above-mentioned causes, accurate history-taking is the key to a correct diagnosis. In this case, the cause of LTN palsy may be sports-related blunt trauma caused by frequent push-ups. LTN palsy is thought to be caused by nerve traction between the fixed points of the scalene muscle and the lower part of the SA muscle.
Patients with LTN injury usually complain of pain or discomfort in the affected shoulder, neck, and scapular area. Symptoms are usually exacerbated by activity, such as tilting the head away from the affected arm and elevating the affected arm. Affected individuals experience shoulder weakness and decreased performance in sports activities [6]. In the early stages, only mild pain may occur during activity; however, if the patient complains of severe pain, further evaluation should be performed to rule out diseases such as neuritis [4,6]. The pain usually subsides within several months, with a typical sign left. The typical sign of SA muscle paralysis is a winged scapula, which can be witnessed by others when the patient is sitting on a chair. The affected scapula is lifted superiorly and toward the spine at rest. When patients flex both arms to a level parallel to their shoulders or use both arms to push a wall, the scapular winging becomes more remarkable [4,6]. Indeed, scapular winging is the landmark manifestation of LTN neuropathy [3]. However, a winged scapula does not always appear in LTN palsy, as in this case. Accurate diagnosis of LTN palsy is based on physical examination, including neurological testing, and a fundamental understanding of the anatomy. EMG is the gold standard for the diagnosis of LTN palsy. However, EMG findings do not predict the functional outcome of LTN neuropathy [8]. Even in severe injuries, clinical function may be restored. Traumatic LTN neuropathy is associated with a poor prognosis compared to idiopathic neuropathy [8].
SA muscle denervation may be seen on MRI, but owing to the small size of the LTN, abnormalities are often missed; however, an abnormal LTN may occasionally be identified on high-resolution MRI [9,10]. In this case, we did not find any abnormalities of the LTN on MRI, whereas EMG helped diagnose LTN palsy.
The differential diagnosis of LTN injury includes cervical disc disease, brachial plexitis, rotator cuff tendinitis or tear, adhesive capsulitis, degenerative arthritis of the glenohumeral joint, degenerative arthritis of the acromioclavicular joint, glenohumeral instability, and thoracic outlet syndrome [6]. We ruled out other causes using plain radiographs of the cervical spine and shoulder, EMG findings, and physical examination. The neurologic causes of scapular winging are LTN injury, spinal accessory nerve injury, and dorsal scapular nerve injury [4,6]. Because of its subcutaneous location, the spinal accessory nerve is quite susceptible to injury. Spinal accessory nerve injury may result in atrophy or paralysis of the trapezius muscle, producing scapular winging clinically [6]. The trapezius muscle is a large muscle that allows for shrugging of the shoulders as well as scapular retraction, stabilization, and rotation. Thus, injury to the spinal accessory nerve can result in scapular winging with the arms in abduction rather than forward elevation. Patients with spinal accessory nerve injury typically have an asymmetric neckline because of the atrophic trapezius and drooping of the shoulder girdle. However, we did not observe the appearance described above in this case. Dorsal scapular nerve injury is characterized by pain along the medial border of the scapula that radiates to the lateral surface of the upper extremities and causes weakness of the rhomboid and/or levator scapulae muscles [11]. Patients with dorsal scapular nerve injury usually complain of ill-defined shoulder pain and dysfunction, with different degrees of functional impairment. The dorsal scapular nerve mainly originates from the fifth cervical nerve root and can become entrapped in the scalenus medius muscle, resulting in rhomboid paralysis. Symptoms of dorsal scapular nerve injury can be resolved by decompressing the dorsal scapular nerve by transecting the scalene muscles. In this case, the tender point was not found in the driving part of the spinal accessory nerve and dorsal scapular nerve. We also found no trapezius palsy or rhomboid palsy. Further, no abnormalities were found on EMG examination of the spinal accessory nerve and dorsal scapular nerve.
LTN palsy usually recovers within 24 months of conservative treatment, such as rest, non-steroidal anti-inflammatory drugs, and physical therapy, including an exercise program [4,6,7]. However, young patients often require active treatment for rapid improvement. Therefore, an SA plane block with US-guided hydrodissection, combined with conservative treatment, can help patients return to daily activities more quickly and improve symptoms. The patient in this case presented with moderate pain and limitation of shoulder flexion and abduction, but no scapular winging. This may be the reason that the patient experienced immediate pain relief and recovered within a relatively short time. In patients with more severe symptoms, such as scapular winging or severe limitation of shoulder motion, the effect of SA plane block with US-guided hydrodissection may be insufficient. In this case, we believe that trauma resulting from overuse and strenuous exercise of the shoulder produced LTN neuropathy. Mondelli et al. [12] reported that only non-traumatic causes were associated with a full or good recovery. However, we achieved good results using the SA plane block with US-guided hydrodissection and believe that this could be a good therapeutic option for LTN neuropathy.
In the management of LTN palsy, it is important to advise patients to avoid activities involving the affected extremity [4,6]. In the acute stage, pain reduction is the major goal, and it is important to modify activities so as not to exacerbate the injury. In the intermediate stage, the pain often subsides as the nerve begins to heal. In the late stage, the SA muscle becomes stronger and shoulder movements improve. Avoiding overstretching the shoulder and gradually increasing activities will help recovery [4,6]. If the symptoms persist, corrective surgery may be needed [4,6,7].
Ultrasound-guided hydrodissection of the peripheral nerve is an effective and safe technique [13-15]. Hydrodissection of a nerve improves its kinematic properties and relieves entrapment. During entrapment, the morphology of the nerve changes, resulting in an alteration/interruption of the flow of axoplasm with eventual fibrosis, increased caliber of the nerve proximal to the site of entrapment, and flattening at the site of entrapment [13,14]. In US-guided hydrodissection, a fluid is injected to separate the nerve from the surrounding structures, which is believed to constrict or irritate the nerve either during movement or at rest. Real-time US is usually the preferred imaging technique in nerve hydrodissection to guide needles and fluid injection. Traditionally, the fluid used for hydrodissection is a large volume of 0.9% normal saline or 5% dextrose [15]. Additionally, a small volume of steroid and local anesthetic solution is injected to reduce pain.