INTRODUCTION
Spinal anesthesia is one of the preferred routes of anesthesia administration for cesarean section [1]. It minimizes the side-effects of drugs on the fetus and provides rapid anesthesia for parturients. However, sympathetic vasomotor blockade effects, such as hypotension, nausea and vomiting, and shivering, can negatively affect the anesthesia experience of the parturient. Moreover, in a previous report of 5,080 cesarean sections in the United Kingdom, 6% of the patients receiving spinal anesthesia did not experience completely pain free anesthesia and required conversion to general anesthesia or additional sedation or analgesia [2]. The role of the anesthesiologist is to provide a safe and comfortable anesthetic experience and help the parturient recover quickly without adverse effects.
Dexmedetomidine is a highly selective α2 agonist and widely used sedative drug during spinal anesthesia that causes sleep-like sedation, opioid sparing analgesia, anxiolysis, and organ protection [3,4]. Intravenous dexmedetomidine has been successfully used in parturients undergoing cesarean section with chronic spinal cord injury [5], as well as tethered cord syndrome [6]. However, dexmedetomidine is generally believed to have side-effects of hypotension and bradycardia [7,8]. Moreover, the simultaneous use of phenylephrine to prevent hypotension during cesarean section adds concerns of bradycardia. In contrast, midazolam is known for its hemodynamic stability and is widely used for sedation during cesarean section. Dexmedetomidine, 0.3 μg/kg, was effective in reducing shivering without hypotension in a parturient after spinal anesthesia during cesarean section. However, this low dose could not provide satisfactory sedation [9].
Here, we tried to evaluate the effect of 0.7 μg/kg dexmedetomidine and compare it with that of 0.03 mg/kg midazolam to maintain sedation equivalent to Ramsay sedation score of 3. This study aimed to compare the efficacy of intravenously administered dexmedetomidine and midazolam for postpartum sedation. We hypothesized that dexmedetomidine would provide better sedation satisfaction than midazolam with similar hemodynamic effects.
MATERIALS AND METHODS
1. Study design
This single-center, prospective, randomized controlled trial was conducted between November, 2021 and October, 2022 at the Nowon Eulji University Hospital. After obtaining approval from the Hospital Review Board (IRB no. 2021-09-018), the trial was registered in the UMIN clinical trial registry (trial identifier: UMIN000053324) prior to patient enrollment. This study was conducted in accordance with the Consolidated Standards for Reporting Trials guidelines.
Informed consent was obtained from all participants. Parturients aged 20-43 years with American Society of Anesthesiology physical status I or II who underwent elective cesarean delivery under spinal anesthesia were recruited. Exclusion criteria included patient refusal, preeclampsia, eclampsia, gestational hypertension, placenta previa, placenta accreta, placental abruption, American Society of Anesthesiology physical status III, multiple pregnancies, contraindications for spinal anesthesia, body mass index (BMI) > 39 kg/m2, and gestational age less than 34 weeks. All the surgeries were performed by a single surgeon.
Demographic data, including age, weight, American Society of Anesthesiology class, comorbidities, gestational age, and history of pregnancy, were collected from all parturients. The investigators and patients were blinded to the group allocation. The patients were randomly assigned to the dexmedetomidine (group D, n = 30) or midazolam (group M, n = 30) group by an independent investigator who was not involved in anesthesia administration. Randomization was achieved using a web-based computer-generated list (www.randomization.com), and the patients numbers were placed in opaque sealed envelopes that were opened in the operating room by an independent anesthesiologist. The anesthesiologist was aware of the allocated group but only followed the anesthetic protocol of our study. Therefore, the data assessors were blinded but the caregivers were not.
2. Anesthetic protocol
All parturients were maintained on a nil per os diet for 8 h prior to anesthesia. Standard monitoring (electrocardiography, noninvasive blood pressure, and pulse oximetry saturation [SpO2]) was performed for each parturient after admission into the operating room. Systolic blood pressure (SPB) was checked at 1 min intervals until the babies were removed and then checked at 5 min intervals. All parturients were treated with prewarmed Hartmann’s solution (10 ml/kg) for 20 min to prevent hypotension. If the blood pressure decreased more than 20% from baseline pressure or the SPB decreased less than 90 mmHg, phenylephrine 50 μg was administered. Subsequently, 25-50 μg phenylephrine was administered according to the parturient’s response to phenylephrine at the anesthesiologist’s discretion. Ephedrine (4 mg) was administered if the heart rate was less than 50 bpm and the SPB was < 90 mmHg. Bradycardia was defined as a heart rate less than 50 bpm. When the heart rate was less than 45 bpm, glycopyrrolate 0.2 mg was administered. Single-shot spinal anesthesia was administered for cesarean delivery. The spinal anesthesia was administered at the L3-L4 interspace. Intrathecal injection of 8-10 mg 0.5% bupivacaine and 10 mcg fentanyl was performed. A pinprick test was used to confirm adequate sensory nerve block at T4-T6. After delivery of the fetus and placenta, 0.1 mg carbetocin was injected, and Hartmann's solution mixed with 10 units of oxytocin was continued at a rate of 30 ml/h. After carbetocin infusion, the patients in group D received 0.7 μg/kg intravenous dexmedetomidine. Group M received 0.03 mg/kg intravenous midazolam. The detailed drug preparation process was as follows. A single investigator responsible for the group assignments prepared the bolus and infused solution of the study drug. For preparation of a bolus of the study drug, either 0.9% isotonic saline (group D) or midazolam (0.03 mg/kg; group M) was diluted in 0.9% isotonic saline to a final volume of 5 ml in a 5 ml polyethylene syringe. For preparation of the loading dose of the study drug, 50 ml of either 0.9% isotonic saline (group M) or 0.7 μg/kg dexmedetomidine (diluted 4 μg per ml) was added in a 50 ml polyethylene syringe, which was labelled as “Loading X”. The loading dose was administered for 10 min.
Sedation was graded according to the Ramsay sedation scale at 10 min interval until the end of surgery. The target maintained sedation level was a Ramsay sedation scale score of 3. After surgery, the parturient was transported to the postanesthetic care unit (PACU). After sensory-level regression was achieved at T10, the parturient was transported to the ward. The parturient was administered intravenous patient-controlled analgesia with 900 μg fentanyl, 100 mg nefopam, and 0.075 mg palonosetron, diluted with normal saline to a total volume 100 ml (continuous, 2 ml/h; bolus, 0.5 ml; lockout 15 min), using a patient-controlled analgesia device for the postoperative 48 h.
3. Outcome measures
Hemodynamic parameters, such as heart rate, systolic blood pressure, SpO2, and tympanic temperature, were recorded as follows: baseline; 5 min after spinal drug injection; baby out; 10 min after study drug administration; 30 min after study drug administration; end of surgery; and 10 min, 30 min, and 50 min after arrival in the PACU. All parameters were recorded by a coinvestigator who did not assign a group allocation and was not involved in the anesthesia practice. The recovery time at the motor level was checked until a modified Bromage Scale score of 2 was achieved. The recovery time of the sensory level was checked until a regression of the sensory level at T10 was obtained.
1) Primary outcomes
The primary outcome was the patient satisfaction score. Patient satisfaction scores were checked for intra- and postoperative experiences 6 h after the ward transfer. Table 1 provides questions regarding sedation during surgery and the experience in the PACU.
2) Secondary outcomes
Secondary outcomes were vital signs, including SBP, heart rate, oxygen saturation, and tympanic temperature, overall vasopressor dosage, incidence of shivering, nausea and vomiting (Table 2), incidence of bradycardia, time to sensory and motor recovery, and postoperative nausea and vomiting (PONV) score and postoperative pain visual analogue scale (VAS) score at 6, 24, 48 h after discharge from the PACU.
4. Statistical analysis
We calculated a sample size of 21 patients for each group based on data from a pilot study of ten cases in each group, as no previous studies were available. In the pilot study, the mean and standard deviation value of satisfaction score in the two predefined groups were 2.8 ± 0.4 and 2.2 ± 0.6, respectively. Thus, the effect size of the two groups was assumed to be 1.18. A sample size of 21 patients was derived for each group, calculated using the Wilcoxon-Mann-Whitney test, two-tailed, with significance level of 0.05, and a power of 0.95 (G power 3.1, Brunsbüttel). This was an exploratory study. For a better estimation of clinical relevance, 30 parturients were enrolled in each group. An independent two-sample t-test was used for normally distributed continuous variables, and data were presented as mean and standard deviation. The Mann-Whitney U test was used to assess patient satisfaction scores. The Fisher’s exact test or chi-squared test was used for categorical variables (incidence of shivering, nausea and vomiting, bradycardia, and hypothermia). A two-way ANOVA with a mixed-effects model was used to analyze the change in SBP, heart rate, SpO2, temperature, and sedation score between the two groups. The GraphPad Prism 9.0 software (GraphPad Inc.) was used for the analysis. Statistical significance was set at P < 0.050.
RESULTS
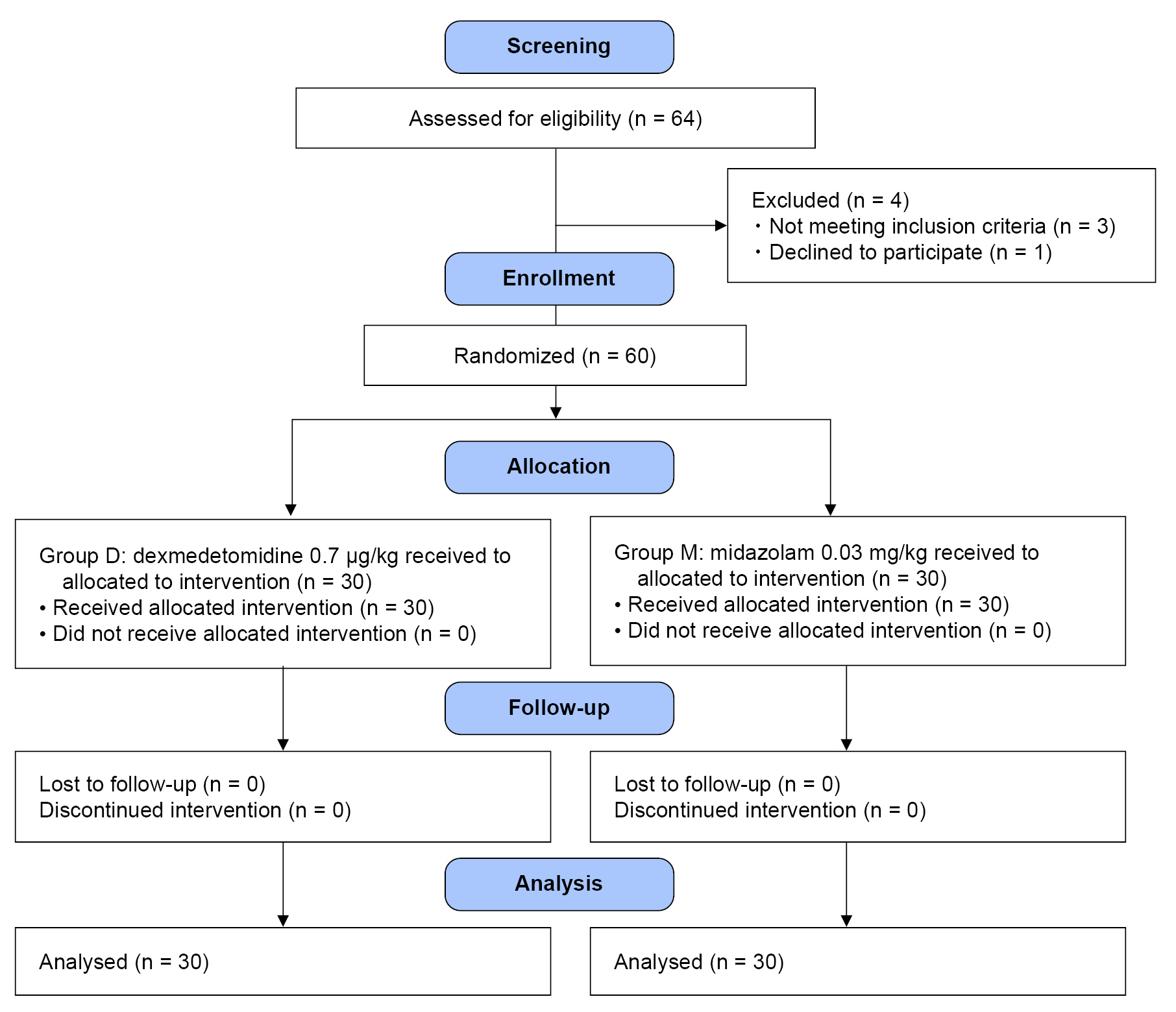
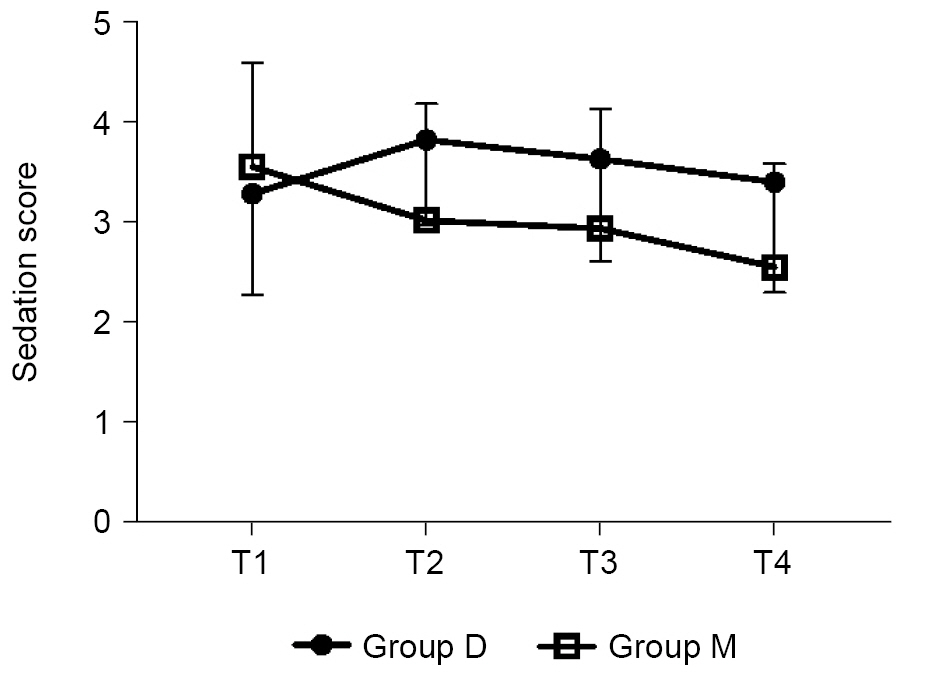
Sixty-four parturients were screened for inclusion in this study. Among them, three parturients did not meet the criteria, and one parturient declined to participate in the study (Fig. 1). Finally, 60 parturients completed the study, and randomization was performed using a computerized method. As a result, 30 parturients each were randomized to the dexmedetomidine (group D) and midazolam (group M) groups. Demographic characteristics (primipara, gestational age, weight, height, and BMI) and duration of surgery were similar between the two groups. The total fluid intake was higher in group D, and the highest block levels were similar. There were no differences in perioperative outcomes (Table 3). There was no significant difference in the median (1Q, 3Q) patient satisfaction scores during surgery or in the PACU (P > 0.050) (Table 4). Satisfaction score for rating the experience during surgery was asked at the time of postoperative 6 h: 15 parturients in group D (50.0%) answered that they slept well during surgery, the other 15 parturients (50.0%) answered they felt sleepful; 11 parturients in group M (36.7%) felt that they slept well, but 4 parturients (13.0%) answered that they could not sleep at all. Regarding the experience in the PACU, 24 (80.0%) and 22 (73.3%) parturients in each group, respectively, answered that they stayed awake and felt comfortable (Table 4). SBP was similar between the two groups. The predicted mean of SBP was 106.3 mmHg in group D and 107.5 mmHg in group M (Fig. 2A). Heart rate was similar between the two groups. Predicted mean of group D was 74 min and that of group M was 77 min; the difference between the predicted means was -3.2 min (Fig. 2B). In addition, vasopressor dosage and bradycardia incidence did not differ between the two groups. Oxygen saturation levels were similar between the two groups (Fig. 2C). Predicted mean oxygen saturation was 99% in both in groups. Temperatures were similar between the two groups (Fig. 2D). Predicted mean temperature of both groups was 36.0˚C. Mean sedation score was 3.2 ± 1.0 in group D and 3.6 ± 1.2 in group M at 10 min after drug administration, whereas, at 30 min after the drug administration, the scores were 3.6 ± 1.0 in group D and 3.0 ± 1.2 in group M (Fig. 3). However, there was no difference in the sedation scores at each time point between the two groups.
For postoperative outcome measures, we evaluated the PONV score and VAS pain at rest, during movement, and at the worst VAS (uterine contraction pain) (Table 5). There were no differences in PONV and VAS scores at postoperative 6 h, 24 h, and 48 h.
DISCUSSION
This randomized controlled study demonstrated that 0.7 μg/kg dexmedetomidine and 0.03 mg midazolam provide similar hemodynamic effects and satisfactory sedation. In addition, there are few side-effects, such as nausea and vomiting, and the same requirement for vasopressor dosage. Parturients in each group had similar postoperative pain scores at rest, during movement, and during uterine contractions. In addition, a low incidence of shivering was observed in both groups.
In this study, we focused on the hemodynamic effects of dexmedetomidine during cesarean section under spinal anesthesia for several reasons.
Dexmedetomidine may induce biphasic hemodynamic alterations. Alpha-2-mediated vasoconstriction may result in transient tachycardia and elevated blood pressure. However, once the baroreceptor is upregulated and the vagal tone is activated, dexmedetomidine may induce hypotension with sympatholytic effects as a result of the reduced release of norepinephrine. In pregnant women, baseline heart rate, stroke volume, and cardiac output are already increased to meet the metabolic demand of the fetus; impairing the compensation of cardiovascular effects may affect parturient's baseline cardiovascular function and cause organ damage [10]. However, in this study, our dexmedetomidine regimen resulted in hypotension similar to that of midazolam during uterine manipulation and placental separation after the baby was removed. The predicted mean SBP was 107 and 106 mmHg in the dexmedetomidine and midazolam groups, respectively. The difference in the mean predicted heart rate between the two groups was only 3 bpm.
It is assumed that a sudden decrease in heart rate is most prominent immediately after spinal anesthesia within 10 min, considering that induction delivery time usually take 5-10 min in the case of uncomplicated cesarean section in our study. In addition, the hemodynamic effect of carbetocin may increase the heart rate, which may affect this finding [11].
Furthermore, our dexmedetomidine dosage was an appropriate option even under a high vagal tone. Only 3 patients among 30 reported bradycardia under 45 bpm and were treated well with ephedrine or atropine after the baby was delivered. However, Kim and Ahn [7] reported a higher incidence of bradycardia when dexmedetomidine was administered during spinal anesthesia. They suggested that initial heart rate was a significant individual predictive factor for the occurrence of bradycardia during dexmedetomidine use [7]. In this study, mean heart rate after baby out in group D was 81.3 ± 12.4. The most profound decrease in the heart rate of dexmedetomidine was observed at 10 min after the loading infusion.
Commonly used sedation agents include midazolam, ketamine, fentanyl, and propofol but the risks from these agents include, but are not limited to, apnea, hallucination, and impaired memory function [12]. Intravenous dexmedetomidine is commonly used for sedation in the nonpregnant patient population through a site in the locus coeruleus and dorsal raphe nucleus; it mimics natural sleep and produces analgesia [13]. Dexmedetomidine is a suitable adjuvant to spinal anesthesia due to its more selective α-2A receptor agonist activity and by acting at the spinal level, laminae VII and VIII of ventral horns. These actions are likely to prolong spinal anesthesia after intravenous dexmedetomidine administration [14]. However, in this study, we did not observe prolongation of the block compared to midazolam. Sivachalam et al. [15] compared the effects of dexmedetomidine and midazolam on the duration of spinal anesthesia and found a prolonged mean time for two dermatomal regressions with dexmedetomidine. We used only the loading dose and measured the sensory recovery time to the T10 sensory level and not the two-level regression time.
Dexmedetomidine increases the frequency of smooth muscle contractions in the uterus [16]. There is a predominance over alpha-2 receptors over alpha-1 in the human myometrium. These effects may have hindered the prolongation of sensory block by dexmedetomidine in our results. Intraoperative dose of 0.7 μg/kg dexmedetomidine for a short duration did not affect the postoperative contraction pain characteristics. Pain scores in both groups were similar. Therefore, parturients experienced similar satisfaction during surgery and during the PACU experience. Therefore, the contraction effect on the uterus, if any, may be temporary and not very large at our utilized dose. Additionally, our dexmedetomidine regimen did not increase the incidence of bradycardia or hypotension. The overall phenylephrine dose was slightly higher in the dexmedetomidine group; however, the difference was not statistically significant. We did not use prophylactic phenylephrine infusion in our study because we tried to measure the effect of blood pressure on each study drug effect. Instead, we used hydration with a crystalloid solution before and during spinal anesthesia.
Xiong et al. [17] reported that ED50 of dexmedetomidine for adequate sedation in postpartum parturients was 1.58 μg/kg, but they made the calculation with the adjusted body weight formula and not exact body weight, and the infusion duration was 15 min; finally, their sedation level was deep, which refers to a observer’s alertness sedation score of less than 3. Hu et al. [18] studied 1 μg/kg of dexmedetomidine and compared its effect with saline or midazolam (0.02 mg/kg). They found equal efficacy in preventing nausea and vomiting after spinal anesthesia.
Our study had several limitations.
First, the sample size calculation was based on our pilot study because there were no similar previous studies. Therefore, future studies with a larger number of patients may be required to confirm our findings. Second, during the loading dose infusion, carbetocin bolus injection was simultaneously administered; therefore, vital signs during the early periods of drug injection may be affected by other factors.
Third, we measured satisfaction scores based on the subjective feelings of sleep during surgery. The objective clinical score of the Ramsay sedation scale indicated satisfactory sedation for almost all patients receiving midazolam and dexmedetomidine, except for two patients in the midazolam group. Patients with pregnancy-induced complications or hypertension were excluded. Therefore, the safety and hemodynamic effects of dexmedetomidine should be tested in high-risk populations.
In summary, intraoperative administration of a loading dose of dexmedetomidine during cesarean delivery produced a similar decrease in SBP and heart rate and a similar satisfaction with sedation. Therefore, an intravenous 0.7 μg/kg dexmedetomidine loading dose is a suitable option for an adjunct drug to provide successful single shot spinal anesthesia.