INTRODUCTION
Postoperative pain causes patients discomfort and vasoconstriction through sympathetic hyperactivity, which may decelerate wound healing and increase the infection rate [1,2]. Therefore, appropriate pain control is important. Proper postoperative pain control reduces morbidity and shortens hospitalization and convalescence [3]. Several factors influence postoperative pain, but depression may significantly heighten its intensity [4,5].
The prevalence of depression is increasing in most countries, including Korea, where the lifetime and annual prevalence are 6.7% and 3.0% [6]. To screen patients with depression, many measures, such as the Patient Health Questionnaire-9 (PHQ-9) [7], Center for Epidemiological Studies Depression Scale [8], Beck Depression Inventory [9], and Geriatric Depression Scale [10], have been developed. However, 30-50% of depressed patients are misdiagnosed due to difficulties in diagnosis [11,12].
Postoperative pain is associated with depression, therefore screening for preoperative depression might help with better management of postoperative pain [4,5]. However, screening for depression in pre-anesthetic assessments is difficult, as it is time-consuming. Moreover, depression screening is difficult for anesthesiologists, as it generally requires professional knowledge. To screen for depression in pre-anesthetic assessments, the screening test should be short, with high reliability and validity. Therefore, PHQ-2 could be an appropriate option, since it evaluates patients using only two of the nine questions of PHQ-9, which is the conventional depression screening test [13].
In this study, we evaluated the usefulness of the PHQ-2 test for preoperative depression evaluation. If there was a correlation between preoperative PHQ-2 and postoperative pain, we considered that PHQ-2 could be used to predict postoperative pain without a definite diagnosis of depression.
MATERIALS AND METHODS
This study was approved by our committee for Clinical Research Ethics (no. KUGH 2017-08-033-006). A total of 55 patients participated in this study. The correlation coefficient of the study was determined to be 0.4, which can be interpreted as a fair result between 0.4 and 0.6, referring to the previous study [14]. The minimum number of samples was 47 when ╬▒ = 0.05, ╬▓ = 0.20, and correlation coefficient is 0.4, and the study was conducted in 55 patients considering the losers. Patients identified as American Society of Anesthesiologist physical status class I-II were scheduled for laparoscopic cholecystectomy under general anesthesia. Patients with a history of depression, current medication, or complaint of post-anesthetic nausea and vomiting in previous surgeries were excluded from this study.
An anesthesiologist, who did not have prior information regarding the patient, visited the ward to examine the PHQ-2 scores of the patients who were hospitalized a day before the operation. Subsequently, he explained the use of intravenous patient-controlled analgesia (IV-PCA). There were two types of PHQ-2: Short-answer PHQ-2 and score-type PHQ-2. In this study, score-type PHQ-2 was used. The PHQ-2 questionnaire consisted of two items: "Little interest or pleasure in doing things" and " Feeling down, depressed, or hopeless." The available answers were: "Not at all," "Several days," ŌĆ£More than half the days,ŌĆØ and "Nearly every day." Each question was scored on a scale of 0-3, and the scores from both questions were added. The patientŌĆÖs medical records (age, height, weight, and history of psychological disorder) were also obtained.
Pre-anesthetic medication was not administered. Propofol (1 mg/kg) and remifentanil (1 ŃÄŹ/kg) were used to induce anesthesia. Anesthesia was maintained using sevoflurane and remifentanil, and remifentanil was discontinued during extubation. In the recovery room, fentanyl 50 ŃÄŹ was administered in the loading dose and IV-PCA was connected. The patient was then told to press the button of the IV-PCA directly if there was pain. An IV-PCA device was used with Hospira Gemstar Blue (GemStarŌäó, Hospira Inc., USA). We mixed 1,000 ŃÄŹ of fentanyl (fentanyl citrate, Hana Pharm, Korea), 50 mg of nefopam (nefopam HCl, Ilsung Pharm, Korea), and 4 mg of ondansetron to obtain a total volume of 150 ml. When the bolus button was pressed, 1.5 ml (10 ŃÄŹ of fentanyl) of the drug mixture was injected. The lock time was 5 min.
The degree of postoperative pain on a numerical rating scale (NRS) and the usage amount of IV-PCA were assessed. The NRS scores were assessed at PACU, 24, and 48 postoperative hours. Usage amount of IV-PCA was collected at 24, 48, and 72 postoperative hours. At 72 h, the IV-PCA device was removed. When a patient complained of nausea or vomited while using IV-PCA, 4 mg of ondansetron was additionally administered. When the complaint sustained, IV-PCA was discontinued.
A statistical analysis was performed using the SPSS (version 24.0, IBM, USA) statistical program. To analyze the correlations among the PHQ-2 score, NRS score, and fentanyl use, point-biserial correlation or Pearson correlation analyses were used. Quantitative variables were expressed as mean ┬▒ SD, and P < 0.05 was the significance level of the test.
RESULTS
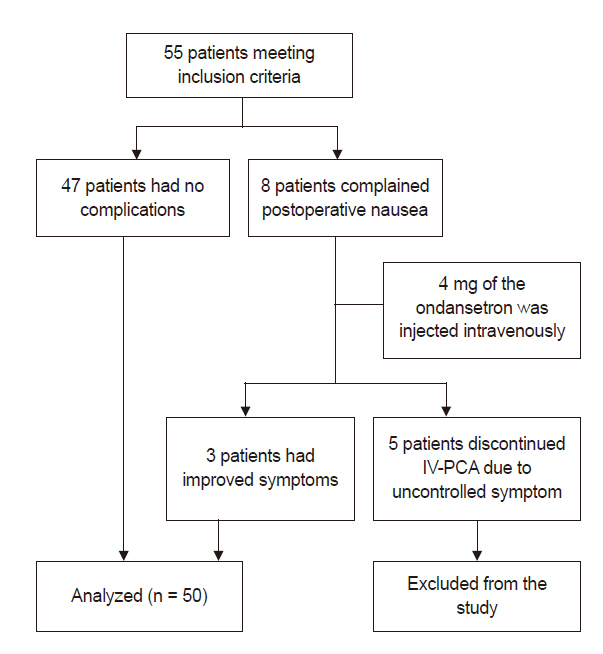
A total of 55 patients who underwent laparoscopic cholecystectomy under general anesthesia were enrolled in this study, of which 8 complained of postoperative nausea and received 4 mg of ondansetron intravenously. Out of the 8 patients, 5 complained of nausea and discontinued IV-PCA due to uncontrolled symptoms after a single administration of 4 mg of ondansetron and were excluded from the study. Finally, we analyzed 50 patients (Fig. 1). Table 1 shows the demographic characteristics. Side effects other than nausea did not occur. In this study, the PHQ-2 was conducted for about two minutes, and no patient refused the survey.
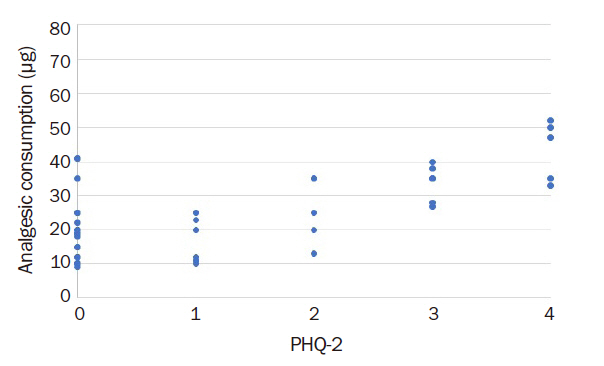
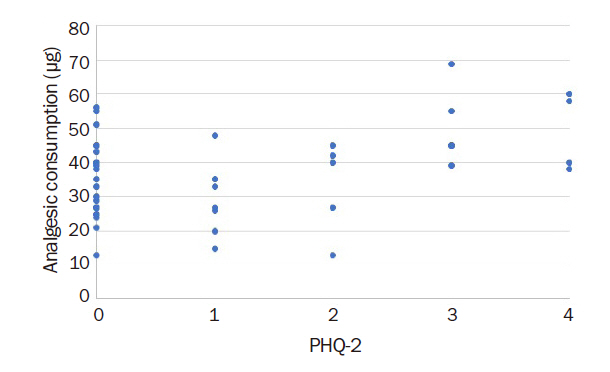
Postoperative NRS in recovery room and total fentanyl usage were not significantly associated with the patient's PHQ-2 score (correlation coefficients: 0.13 [P = 0.367] and 0.24 [P = 0.098], Table 2). When three points on PHQ-2 was used as the cut-off score, the fentanyl use was significantly higher in patients who scored Ōēź 3 points than in those scoring < 3 points (371.6 ┬▒ 71.5 vs. 300.3 ┬▒ 88.6), and total fentanyl usage correlated with the PHQ-2 score (correlation coefficients: 0.33 [P = 0.018]). Fentanyl usage at 24 and 48 postoperative hours were significantly associated with the PHQ-2 score (correlation coefficients: 0.68 [P < 0.001] and 0.45 [P = 0.010], Table 2). Figs. 2, 3, and 4 show the relationship between PHQ-2 score and analgesic consumption on first, second, and third day after surgery. Age was associated with total fentanyl usage but sex was not (correlation coefficients: -0.34 [P = 0.016] and -0.69 [P = 0.640], Table 2). ŌĆā
DISCUSSION
The purpose of this study was to evaluate the correlation between preoperative PHQ-2 score and postoperative pain. PHQ-2 is a simple screening test using two of the nine questions of PHQ-9, a previously developed depression screening test [13]. The two questions addressed depressed mood and anorexia. There is a significant correlation with other screening tests, and PHQ-2 is known to increase the total score depending on the severity of depression in the patient group [15].
In this study, the preoperative PHQ-2 scores did not significantly correlate with the postoperative NRS scores measured in the PACU or the total fentanyl usage (correlation coefficients: 0.13 [P = 0.367] and 0.24 [P = 0.098]). However, fentanyl usage during 24 postoperative hours highly correlated with the preoperative PHQ-2 scores (0.68 [P < 0.001]). Various studies on the association between postoperative pain and preoperative depression have been conducted. De Cosmo et al. [14] reported that depression was associated with tramadol use in patients after laparoscopic cholecystectomy. Schade et al. [16] reported that preoperative depression affects postoperative pain and rehabilitation in patients with lumbar disc herniation. Oztekin et al. [17] reported that anterior cruciate ligament surgery was not associated with postoperative pain despite high preoperative depression scores in the patients. Kavakci et al. [18] found that preoperative anxiety has a greater impact on postoperative pain compared to depression in cases of ear, nose, and neck surgery. These differences are probably because of differences in the type of surgery and type of postoperative analgesics used.
Patients who were included in this study underwent laparoscopic cholecystectomy. The surgery was less painful compared to open cholecystectomy, and IV-PCA with fentanyl controlled postoperative pain appropriately [19]. Immediately after the surgery, patients with higher PHQ-2 score had higher analgesic requirements. However, as the postoperative pain was controlled with a strong opioid, the appropriate pain control effect might have been achieved regardless of the PHQ-2 score, and it is believed that there was no difference in usage.
PHQ-2 scores did not significantly correlate with total fentanyl usage. However, after selecting the appropriate cut-off score for PHQ-2, the PHQ-2 scores were associated with total analgesic requirement. The sensitivity and specificity of depression were 91.9% and 100%, respectively, when the cut-off score on PHQ-2 was 3 [15]. In this study, when 3 points were used as cut-off score, fentanyl use was significantly higher in patients who scored 3 or more points. Therefore, 3 points as a cut-off score on PHQ-2 may be appropriate for preoperative depression screening.
In this study, sex did not affect analgesic use (correlation coefficient: -0.69 [P = 0.640]). In another study on analyzed factors affecting postoperative pain, sex did not affect the postoperative pain or analgesic use [4]. However, age was a major predictor of postoperative pain and analgesic use [4]. In this study, the use of analgesics was higher in younger patients (correlation coefficient: -0.34 [P = 0.016]).
This study has a few limitations. First, anxiety was not investigated. Anxiety plays a major role in acute pain, including postoperative pain [18]. Brander et al. [20] reported that depression had a greater effect on postoperative chronic pain than anxiety. Patients' anxiety before surgery should have been examined to confirm its association with pain. Second, the diagnosis of depression was not an inclusion criterion. Therefore, in a controlled study on patients who were diagnosed or treated for depressive disorders, we intend to assess the efficacy of PHQ-2 as a predictor of postoperative pain. Marazziti et al. [21] reported that in the group with depression, the pain threshold was lower than in the group without depression. Depressed patients who had lower thresholds for postoperative pain were believed to have higher analgesic requirements and more negative effects of pain. Future studies could evaluate pain control or patient satisfaction when controlling postoperative pain more aggressively by increasing the amount of pain medication IV-PCA in patients with high PHQ-2 scores.
In conclusion, the PHQ-2 test is composed of two simple questions and can be performed in two minutes; therefore, it could be useful as a screening test for preoperative depression. Despite the simple questions, it highly correlated with fentanyl consumption in the early postoperative period. Particularly, when 3 points were used as the cut-off score, the PHQ-2 score was associated with the dosage of analgesics, and the analgesic demand could be expected to be high with higher PHQ-2 scores.