Risk factors for postoperative delirium in elderly patients after spinal fusion surgery
Article information

Abstract
Background
Postoperative delirium (POD) has an incidence rate of 9% to 41%. It is directly linked to decreasing cognitive function, increasing length of hospitalization and cost, as well as other complications and mortality. We aimed to assess the risk factors for POD among elderly patients by analyzing data from those who underwent spinal surgery.
Methods
This study included 446 patients aged 65 years or older who underwent spinal surgery at our institution between March 2013 and May 2018. Data were collected retrospectively from the patients’ electronic medical records, and logistic regression was used to identify the risk factors associated with POD. The diagnosis of POD was based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, and was made through consultation with a psychiatrist during postoperative hospitalization and before discharge.
Results
Seventy-eight (78/446, 17.4%) patients were diagnosed with POD. The most relevant risk factor for POD was preoperative cognitive dysfunction (odds ratio [OR], 4.37; 95% confidence interval [CI], 1.60 to 11.93; P = 0.004), followed by emergency surgery (OR, 2.70; 95% CI, 1.27 to 5.74; P = 0.01), age (OR, 1.19; 95% CI, 1.13 to 1.26; P < 0.001), and anesthesia time (OR, 1.01; 95% CI 1.00 to 1.01; P = 0.002).
Conclusions
Preoperative cognitive dysfunction, emergency surgery, age, and anesthesia time were factors that affected POD occurrence after spinal surgery. Patients with such associated factors may be at a higher risk for POD when undergoing spinal surgery, and hence, careful management may be necessary for these patients.
INTRODUCTION
With an increase in the global elderly adult population, the number of surgeries being performed on elderly patients has been increasing. In Korea, the number of spinal surgeries performed has increased over the years, from 110,000 in 2007 to 170,000 in 2013, and it is the fourth most common surgery among 33 major single surgeries. In particular, the frequency of spinal surgery in patients aged over 65 years has increased from 0.9% in 2007 to 1.3% in 2013. Spinal-surgery-related costs are also high, ranking fifth for hospitalization and sixth for outpatient care [1].
Postoperative delirium (POD) is one of the most common postoperative complications in elderly patients. Its incidence varies from 9% to 41%, depending on the type of surgery or timing of POD assessment [2,3]. In Korea, Shin et al. [4] reported a POD incidence of 36.5% among elderly (> 65 years old) patients undergoing gastrectomy. Other researchers reported POD incidences of 21.4% among elderly (> 70 years old) patients undergoing neurosurgical surgeries [5], 22.7% among elderly (> 65 years old) patients undergoing cardiac surgery, and 6.7% among elderly (> 60 years old) patients undergoing orthopedic surgery [6,7].
POD is associated with decreasing cognitive function, increasing hospitalization cost and duration, and increasing complications and mortality [8,9]. Preventing POD, or reducing its incidence, is important for improving a patient’s prognosis. POD is described as a multifactorial syndrome [10]. Perioperative active control of these factors would be the best way to improve outcome. For example, Marcantonio et al. [11] could lower the incidence of POD by conducting geriatric consultation according to their protocol during the hospitalization period.
The known risk factors for POD include age [12], impaired functional status, preexisting dementia [13], and preexisting cognitive impairment [14]. Because these risk factors were determined on the basis of the analysis of various types of surgeries, questions remain about their generalizability and application to patients undergoing spinal surgery. Only a few studies have focused on the spinal area or risk factors for delirium following spinal surgery [9,15–17].
Various studies have reported different incidences of POD, and an important factor causing this difference is the type of surgery [2–7]. Although these studies were conducted on similarly aged elderly patients (65 years or older), the reported incidences of POD varied according to the type of surgery, thus indicating the need for considering another risk factor. Health insurance reports show that the frequency of spinal surgery is increasing in this age group, and as a result of the rapidly increasing elderly population in Korea, the frequency of POD among elderly patients who have undergone spinal surgery is also expected to increase [1]. Since little research has been conducted on this patient group, we performed this study with an aim of providing evidence for their clinical care.
Moreover, most studies have analyzed only simple POD incidence reports or the presenting general risk factors from the surgeon’s perspective [9,18]. Therefore, we also aimed to investigate the possibility of preventing or reducing POD incidence by exploring reversible risk factors from the anesthesiologist’s perspective. In this study, we compared the characteristics of elderly patients with delirium after spinal surgery to those of normal patients. In addition, we examined the risk factors contributing to POD to identify factors that can be adjusted during the perioperative period.
MATERIALS AND METHODS
After receiving approval from the Institutional Review Board (no. SGPAIK 2018-08-023), this study was conducted by retrospectively reviewing the electronic medical records (EMRs) of 458 elderly patients who underwent spinal surgery at our institution between March 2013 and May 2018. We included patients (1) who were 65 years and older [16,18,19] (2) who had undergone spinal fusion surgery (3) involving more than two segments (4) under general anesthesia. We excluded patients who had undergone more than one surgery during hospitalization (n = 12). Therefore, the final study population included 446 patients.
Immediately before the surgery, intravenous glycopyrrolate (0.004 mg/kg) was administered as a premedication. During the surgery, general anesthesia was maintained using volatile or intravenous anesthetics. Intravenous anesthetics were used when motor-evoked potential monitors were employed. If postoperative intensive care unit (ICU) admission was required, the patient was transferred immediately after surgery. For postoperative analgesia, fentanyl (1 μg/kg) was routinely administered intravenously 15 min before completing skin suturing. If a patient’s numerical rating scale (NRS) score in the recovery room was more than 5 points, he/she was given additional fentanyl (1 μg/kg), and the process was repeated until the NRS score fell below 4 points. Once the patient returned to the ward, patient-controlled analgesia (PCA; a mixture of nefopam hydrochloride [80 mg], ramosetron hydrochloride [0.6 mg], and normal saline [88 ml]) was used for a maximum of 3 days. PCA was set up to enable a bolus shot (1 ml) with a 15-min lock-out time and a 1-ml/h basal rate.
The data were extracted from the EMRs generated at the time of hospitalization. The data included demographic data (age, sex, height, and weight), American Society of Anesthesiologists physical status class, alcohol (frequency per month) and smoking history (pack-year), various comorbidities (cardiac, pulmonary, renal, hepatic, neurologic, etc.), use of anticoagulants, preoperative laboratory test results (hemoglobin, albumin, sodium, and creatinine levels), waiting days from admission to surgery, and the emergency status. Preoperative comorbidities and medication were assessed and verified using preanesthetic assessment and consultation records.
Comorbidities were organized into independent risk factors according to cardiovascular (hypertension, angina, ischemic heart disease, heart failure, cardiomyopathy, valve disease, or arrhythmia), respiratory (chronic obstructive pulmonary disease, pulmonary edema, pleural effusion, atelectasis, or pneumonia), and hepatic (hepatitis or liver cirrhosis) diseases. Patients with a present illness of acute kidney injury or chronic kidney disease with or without dialysis before surgery were defined as having the risk factor “renal failure.” Preoperative cognitive dysfunction (dementia or Parkinson’s disease) and delirium were identified using psychiatric consultation records and medical history. In addition, the duration of anesthesia (min), events of hypothermia (< 36.0℃), amount of intraoperative bleeding (ml), amount of infused fluid (ml), volume of intraoperative blood transfusion (ml), and frequency of pressor agent administration (5 mg bolus of ephedrine intravenously or 50 μg bolus of phenylephrine intravenously) were explored. If a patient showed symptoms of delirium after surgery during hospitalization, the attending physician consulted with a psychiatrist for the diagnosis and treatment of POD. The psychiatrist made the diagnosis based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition if a patient had any suspicious symptoms, such as poor behavioral control, unawareness, or decreased alertness. However, tools such as the Delirium Rating Scale-Revised-98 were not applied to assess the severity of symptoms.
We also explored other postoperative outcomes related to POD, including the rate of ICU admission, days of ICU admission, days of hospital admission, and mortality.
Statistical analysis
The data were presented as the mean ± standard deviation or number of patients (percentage). Continuous-type risk factors (e.g., days of hospital admission, age, body weight, height, anesthesia time, or transfusion/bleeding volume) were compared between the two groups by using Student’s t-test or the Mann–Whitney U test, based on the results of the Shapiro–Wilk normality test. The incidence of mortality and comorbidities was compared between the groups by using the chi-squared test.
A logistic regression analysis based on a binomial generalized linear model was performed to identify the risk factors associated with POD. To identify significant independent risk factors for POD, univariate (cutoff value was P < 0.1) and multivariate logistic regression analyses were used. Independent risk factors with P < 0.05 in the multivariate analysis were considered statistically significant. For producing the final logistic regression model, the risk factors were selected by weighting the clinical implication rather than the statistical values. The C-statistic and Hosmer–Lemeshow goodness-of-fit test were used to assess the fitness of the logistic regression model. All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., USA).
RESULTS
Of the 446 patients, 78 (17.4%) were diagnosed with POD. The differences in patient characteristics, preoperative anesthetic evaluation data, and intraoperative factors between the non-POD and POD groups are shown in Table 1. The POD group showed older age (P < 0.001) than did the non-POD group. The POD group showed a greater incidence of comorbidities, including diabetes mellitus (P = 0.013), renal failure (P = 0.009), preoperative delirium (P = 0.009), and preoperative cognitive dysfunction (P = 0.001). They also had a significantly greater rate of emergency surgery (P = 0.023) and more delayed surgery (P = 0.014). Moreover, they showed lower preoperative hemoglobin level (P = 0.007), more frequent preoperative hyponatremia (P = 0.003), hypoalbuminemia (P = 0.002), and high serum creatinine level (P = 0.042). Total anesthesia time was also longer in the POD group (P = 0.021).

Comparison of Demographics and Characteristics of Patients with/without Postoperative Delirium
The results of univariate logistic regression analysis are presented in Table 2. As preoperative risk factors for POD, the significant relevant factors were age (odds ratio [OR], 1.18; 95% confidence interval [CI], 1.12 to 1.25), emergency surgery (OR, 2.27; 95% CI, 1.17 to 4.39), diabetes mellitus (OR, 1.94; 95% CI, 1.17 to 3.20), renal failure (OR, 6.05; 95% CI, 1.80 to 20.36), preoperative delirium (OR, 6.23; 95% CI, 1.63 to 23.77), and cognitive dysfunction (OR, 4.67; 95% CI, 1.83 to 11.91). The significant relevant factors in the preoperative laboratory data for POD were hemoglobin level (OR, 0.80; 95% CI, 0.68 to 0.95), hyponatremia (OR, 2.68; 95% CI, 1.43 to 5.02), hypoalbuminemia (OR, 3.02; 95% CI, 1.55 to 5.88), and high level of serum creatinine (OR, 2.35; 95% CI, 1.10 to 5.03). Anesthesia time was a significant intraoperative factor (OR, 1.00; 95% CI, 1.00 to 1.01).

The Results of Univariate Logistic Regression Analysis for Postoperative Delirium
The most important risk factor as revealed by the complete logistic regression analysis was preoperative cognitive dysfunction (OR, 4.37; 95% CI, 1.60 to 11.93; P = 0.004). Emergency surgery (OR, 2.70; 95% CI, 1.27 to 5.74; P = 0.01), age (OR, 1.19; 95% CI, 1.13 to 1.26; P < 0.001), and anesthesia time (OR, 1.01; 95% CI, 1.00 to 1.01; P = 0.002) were also associated with POD (Table 3).

Final Logistic Regression Model for the Risk Factors of Postoperative Delirium in Elderly Patients after Spinal Fusion Surgery Using Independent Risk Factors Obtained through Univariate Analysis
Other postoperative outcomes related to POD are shown in Table 4. The POD group showed a significantly higher incidence of ICU admission (P = 0.003) and longer ICU stay (P = 0.011) than did the non-POD group. They also showed 0.6 times longer total hospital stay (mean days, 25.7 days vs. 41.2 days) and 3.7% higher mortality (1.4% vs. 5.1%).
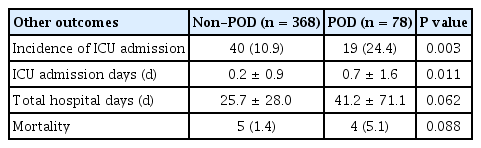
Major Postoperative Outcomes related Postoperative Delirium
DISCUSSION
In this study, the incidence of POD was 17.4%, and the associated risk factors were preoperative cognitive dysfunction, emergency surgery, age, and anesthesia time. POD was associated with increased mortality, higher incidence of ICU admission, and longer length of admission.
The incidence of POD in this study was similar to that (11.8%) reported by Fineberg et al. [9] who evaluated the risk factors for POD in 570,000 patients who underwent lumbar decompression surgery or lumbar fusion. However, Brown et al. [17] reported a much higher POD incidence of 40.5%. These differences in POD incidence seem dependent on the diagnostic methods used. Since our patients were diagnosed via psychiatric consultations when symptoms developed, some patients with milder symptoms may have been missed during this process. To provide accurate diagnosis and appropriate treatment for POD, delirium evaluation may need to be performed as a routine practice in high-risk patients, and not just in symptomatic patients.
The cause of delirium is multifactorial and has been attributed to numerous risk factors. Age is the most frequently identified risk factor for POD, and other risk factors include preexisting dementia, preoperative anemia, drug or alcohol abuse, large intraoperative blood loss, duration of surgery, general anesthesia, electrolyte imbalance, high average pain, and frequent hypotension [9,15,16]. In this study, we identified that preoperative cognitive dysfunction, emergency surgery, age, and anesthesia time were significantly associated with POD (Table 3). Age is a known factor closely related to the incidence of POD [15,20], and in this study, the mean age of the POD group was significantly higher than that of the control group (76.4 years vs. 72.2 years; P < 0.001). Katznelson et al. reported that age older than 65 years was associated with a threefold increased risk of POD [21]. The higher incidence of POD in the elderly may be associated with increased comorbidities as well as age-related neurobiological changes (e.g., reduced brain volume and weight, and decreased production of cerebral neurotransmitters).
Prolonged anesthesia time can be interpreted as another representation of the duration of surgery time, and it is a known risk factor according to previous studies [15,16]. Prolonged surgery time may indicate more complex procedures with increased exposure to microemboli and the systemic inflammatory response [22].
Previous studies have shown that preoperative cognitive dysfunction is highly relevant, but its incidence varies depending on the type of surgery [23,24]. In this study, cognitive dysfunction was evaluated across cases of preoperative dementia, Alzheimer’s disease, and delirium. The cholinergic system and somatostatin are essential for normal cognitive function, attention, and the sleep-wake cycle, and their deficiency can cause dementia [25]. Therefore, patients with dementia are more vulnerable to delirium.
The relationship between emergency surgery and POD is still controversial. Ansaloni et al. [26] suggested that emergency surgery is related to POD, even though this was not supported by multivariable analysis. Moreover, they reported a significantly higher (11%) incidence of POD in an emergency setting, which was similar to our results (19.2% vs. 9.2%, P = 0.023). They attributed this finding to the fact that emergency surgery did not entail environmental conditions that made patients feel comfortable. However, Malik et al. [27], who assessed the risk factors for delirium in cases of femoral fractures, reported higher POD incidence in non-emergency surgeries. In emergency surgeries, the risk factors for POD will be clear, as these surgeries can be performed without treating various correctable risk factors. However, this is difficult to interpret because the risk factors for POD have multiple causes, and non-drug treatments, such as those for ensuring patient comfort, cannot be completely excluded in an emergency situation. Therefore, further study is warranted on this point.
As is well known, POD has a significant effect on various postoperative outcomes [17,28]. Patients with POD have 3.9 times higher mortality rates and 2.6 times higher rate of ICU admission than do those without POD. Moreover, they showed more prolonged ICU admission and hospital admission (Table 4). In other words, POD negatively contributes to the prognosis of patients and is closely related to increasing medical costs. Therefore, identifying the risk factors for POD is important.
The risk factors for POD identified in this study are similar to those reported previously; nonetheless, there are some limitations to generalizing these results. This is because the study was conducted on patients from a single medical institution in Korea. A comprehensive analysis of patients from multiple centers will be needed in the future. Another limitation is that patients with mild symptoms of POD may not have been diagnosed because the attending physician requested psychiatric consultation only if the patient had clear delirium symptoms. This has an advantage in the analysis based on a solid diagnosis, but the low rate of diagnosis may have affected the analysis of the association among risk factors. In addition, patients who showed POD symptoms after discharge were not diagnosed and might have been omitted. Lastly, the severity of delirium could not be analyzed because the severity of delirium and cognitive dysfunction was not classified. This is a drawback of the diagnosis process. Patients with mild symptoms are often excluded from the diagnosis process, and analysis of the difference between risk factors and prognosis according to the severity of symptoms is not carried out. Therefore, to address these limitations, large-scale studies on more patients are needed.
In summary, this study confirmed that preoperative cognitive dysfunction and age were associated with POD after spinal fusion surgery, along with emergency surgery and anesthesia time. Although cognitive dysfunction and age cannot be modified, they can be used as predictors for POD. In patients who need emergency surgery, efforts to reduce the risk of POD through prior evaluation, stabilization of patients, and sufficient explanation of surgery may be beneficial.
Acknowledgements
This work was supported by the 2012 Inje University research grant.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Sijin Choi, Byunghoon Yoo, Sangseok Lee, Mun Cheol Kim. Data acquisition: Sijin Choi, Inyoung Jung, Sangseok Lee. Formal analysis: Sijin Choi, Byunghoon Yoo, Sangseok Lee. Funding: Mun Cheol Kim. Writing-original draft: Sijin Choi, Inyoung Jung, Byunghoon Yoo, Sangseok Lee, Mun Cheol Kim. Writing-review & final proofing: Sijin Choi, Inyoung Jung, Byunghoon Yoo, Sangseok Lee, Mun Cheol Kim.