INTRODUCTION
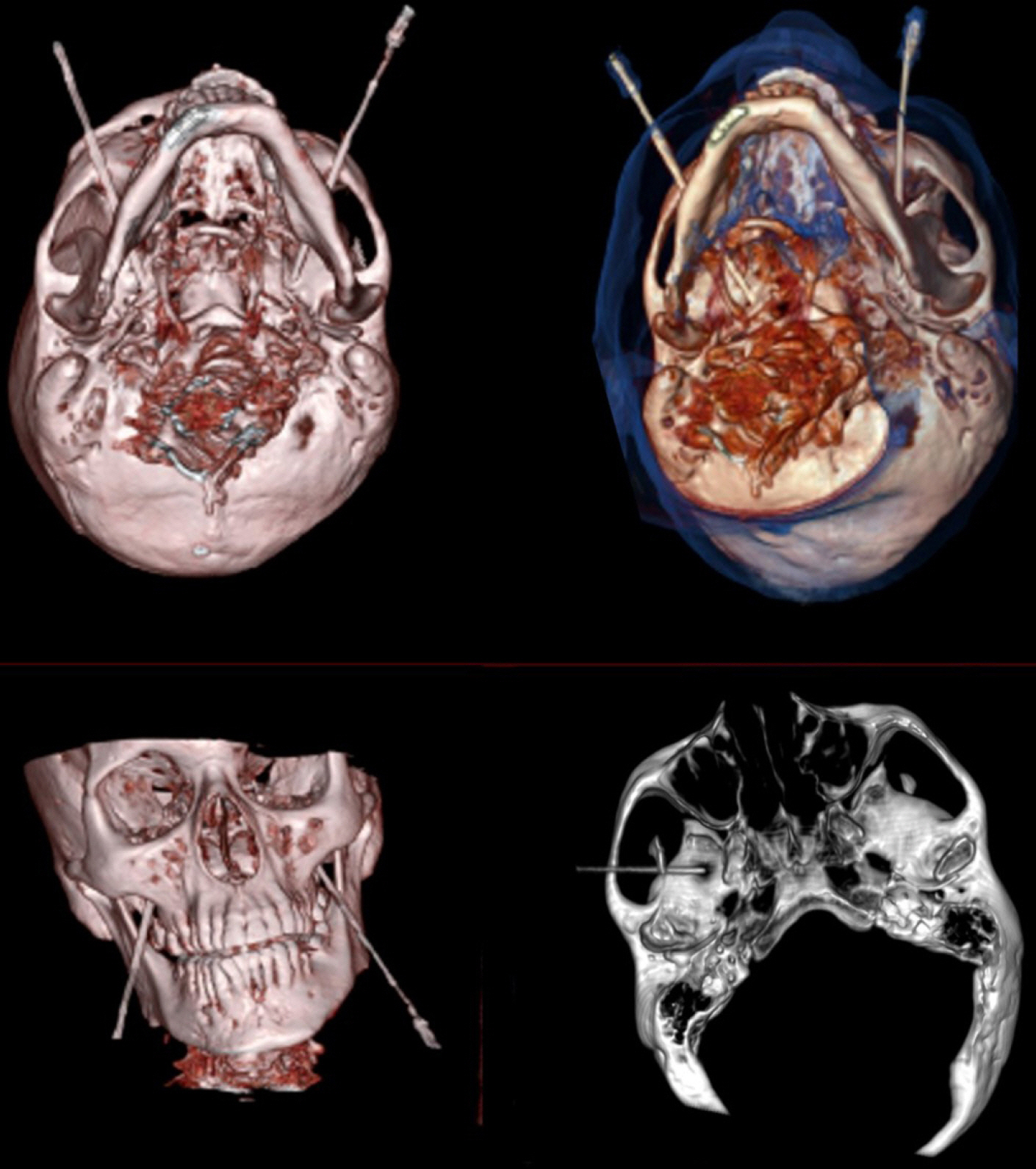
Eighty percent of patients with head and neck cancer complain of facial pain [1]. Pain in these settings may result directly from the tumor or as a side effect of oncological treatment in the form of radiotherapy, surgery, or even chemotherapy. Additionally, cancer progression and treatment can sometimes lead to anatomical deformations that complicate interventional therapy (Fig. 1).
Although oncological facial pain is mainly related to head and neck tumors, intracranial and, rarely, distal tumors may present with similar symptoms. These include headache, trigeminal neuralgia, trigeminal autonomic cephalalgia, and orofacial pain. Additionally, distal tumors may present with neuropathies [2]. Most of the time, these patients present with trigeminal-like pain; therefore, the Gasserian ganglion is an instrumental target for interventional pain management in this population.
For trigeminal neuralgia pain, evidence recommends microvascular decompression (very weak), stereotactic radiosurgery (weak), radiofrequency treatment of the Gasserian ganglion (weak), and pulsed radiofrequency (very weak) [3-5]; the common sequence includes a previous diagnostic block. For patients with cancer, the literature supports the use of neurolytic agents [6]. Furthermore, some studies have included peripheral approaches to distal branches [7].
The foramen ovale approach can be a difficult and time-consuming interventional procedure for physicians, requiring precision to place the needle. Moreover, suboptimal needle positioning can lead to treatment failure, recurrence, and potential complications, including nonspecific block, intracranial hemorrhage, subarachnoid injection, and infections [8,9].
Some authors have reported a successful stereotactic approach combined with a three-dimensional computed tomographic reconstruction model to improve accuracy, safety, and efficiency [10]. We share our experience with computed tomography (CT) guidance Gasserian ganglion interventions and their role in treating cancer-related facial pain in patients with complex anatomy.
MATERIALS AND METHODS
Study design
This observational, retrospective study was conducted at the National Cancer Institute of Mexico City. Approval was obtained from the institutional review board (2019/0097). The requirement for written informed consent was waived owing to the retrospective nature of the study.
Data collection
A review of the electronic medical records at the Instituto Nacional de Cancerologia pain clinic was conducted from January 1, 2015, to December 30, 2018, at the National Cancer Institute. We included patients over 18 years of age diagnosed with cancer-related facial pain confirmed by magnetic resonance imaging, refractory to medical treatment, with a numerical rating scale (NRS) over 5 points, and who underwent a CT-guided Gasserian ganglion intervention. Patients with mental disorders, poor documentation, or other causes of pain were excluded.
Variables
The following data were collected from the patient charts: age; sex; tumor type; side (left, right, or bilateral); affected branch (V1, V2, V3, or combination); drugs used for the intervention (local, steroids, phenol); and time of radiofrequency. We monitored intra-and postoperative complications including corneal anesthesia or loss of corneal reflex, blindness, facial dysesthesia, masseter weakness, cerebrospinal fluid leakage, carotid-cavernous fistula, and perioperative death. Patient satisfaction was evaluated on a Likert scale (unsatisfied to very satisfied).
We collected outcome data regarding pre- and post-procedural status, NRS 0-10, and the douleur neuropathique 4 (DN4) questionnaire. Satisfactory pain relief was defined as a reduction of 3 points in the NRS and DN4 scores for at least 7 days.
Gasserian ganglion intervention technique
All procedures were performed by experienced pain physicians in CT rooms in the supine position under standard sedation (2 µg/kg fentanyl and 0.075 mg/kg midazolam). The puncture was performed according to the Hartel anatomical landmarks for percutaneous procedures. The head was positioned supine and rotated slightly away from the puncture side. The entry point was 2.5 cm lateral to the mouth angle (Fig. 2). After skin preparation and local anesthesia, a 22-G (32 mm) needle was introduced into the foramen ovale, and a 128-slice spiral CT Siemens Flash scan was used to confirm the needle position. After verification, medical treatment was administered to each patient as follows: radiofrequency, 10% phenol, bupivacaine, or steroids (dexamethasone). All patients were closely-monitored for 2 h and reevaluated 7 days later.
Statistical analysis
Data distribution was determined using the Kolmogorov-Smirnov test. Categorical data were described as percentages and continuous data as medians and standard deviations. A paired sample t-test (with a cut-off of P < 0.05 for statistical significance) was used for outcome comparison. All statistical analyses were performed using SPSS Version 25.0 (IBM Co.).
RESULTS
A total of 32 patients were initially screened, and 24 were included in the final analysis: 70% female and 30% male, respectively. The mean age was 56.6 ± 13.5 years. The right side was affected in 58.3% of the cases, and a combination of branches, specifically V2 + V3, was the most common presentation (75%). More than 8% of interventions were performed bilaterally. The most common neoplasms were head and neck tumors (83.3%) (Table 1). Neurolysis was performed with phenol in 37.5% of patients, and radiofrequency was performed in 33.3%, with a median time of 180 (120, 360) s (Table 2).
Most patients (95.8%) had favorable clinical outcomes. After the procedure, 70.8% of the patients were satisfied, 16.7% were very satisfied, and 12.5% were unsatisfied. Facial dysesthesia was the only complication reported by 8.3% of patients (Table 3). We observed a significant reduction in NRS and DN4 scores from 7.6 ± 1.4 and 4.4 ± 1.4 to 3.2 ± 2.0 and 2.2 ± 1.4 points, respectively (P < 0.001) (Table 4). when looking at complications separated by intervention; this was observed in the phenol plus radiofrequency group (Table 5).
DISCUSSION
Hartel first described the treatment of trigeminal neuralgia with absolute alcohol through a percutaneous foramen ovale approach to the Gasserian ganglion in 1912 [11]. However, the efficacy and safety of percutaneous interventions depend mainly on the precision of the target. When using fluoroscopy, it may be challenging to visualize the foramen ovale, as soft tissues and blood vessels cannot be visualized. This is especially relevant for patients with cancer, as the anatomy is often disturbed by tumor progression, radiation, chemotherapy, or surgery. CT is a useful tool for identifying the optimal position and predicting intraoperative difficulties. Although previous studies on CT reconstruction for difficult-to-access foramen ovale interventions have been published [10], no study has been performed in an oncological population with complex anatomy, including bilateral approaches.
The present study showed a significant reduction in NRS (7.6-3.2; P < 0.001) and DN4 (4.4-2.2; P < 0.001) scores and most patients reported being satisfied. Our results are consistent with those of previous studies [10-14]. Regarding clinical presentation, we obtained similar results, with the right branch being the most affected, specifically V2 + V3 [15,16]. We also agree with previous studies on the etiology of pain, where head and neck tumors were the most frequent [1,2].
Regarding treatment options, we opted for phenol, not glycerol, because of accessibility in our hospital; nevertheless, phenol 10% has been described as a valuable option, especially in patients with cancer [17]. There is still controversy regarding the optimal administration of radiofrequency therapy. However, most studies suggest lesions at a maximum of 0.5 V, 75 cycles/s at 55 to 80°C for 120 s; we presented a median time of 180 s [17,18].
Unlike previous studies, we included patients with bilateral pain treated with chemical neurolysis, which demands a higher anatomic understanding and skills. Nevertheless, similar to these studies, we reproduced an effective and safe CT-guided technique [12-14]. We achieved 100% technical success with appropriate needle positioning with a significant reduction in pain. In contrast, Telischak et al. [14] reported minor complications, such as throat numbness, which can be explained by the combined approach of the Gasserian and glossopharyngeal nerves. Zheng et al. [12] reported that facial dysesthesia was the most common complication. This was the only complication reported in our patients. There are two explanations for this: a short follow-up time and a more precise location with 3D reconstruction, which was presented in patients with significant anatomical deformations.
Two previous meta-analyses [19,20] concluded that puncture guidance technology has an absolute advantage in puncturing the foramen ovale, can improve the one-puncture success rate, learning curve, and safety, and can reduce the incidence of complications and operation times. We reproduced this in an oncological population with complex anatomy using CT guidance.
Limitations
The present study had certain limitations inherent to a retrospective, single-center investigation. The survival of patients with cancer can explain our limited sample size; in addition, only patients with complex anatomy were included. We did not evaluate the results in terms of quality of life, and associated or secondary symptoms, such as anxiety or depression, were not investigated. Additionally, the follow-up was very short; therefore, we could not monitor late complications.
Conclusions
To the best of our knowledge, this is the first study performed on a cancer patient population using bilateral approaches. Our data suggest that CT guidance is a safe tool for interventional physicians treating facial pain in cancer patients with complex anatomy. Therefore, we do not recommend using only fluoroscopic guidance techniques in patients with head and neck cancer who have previously undergone surgery or have other causes of intricate anatomy. Accordingly, our algorithm includes a recent CT and magnetic resonance imaging and the use of local anesthetic as an initial treatment. If pain relief is significant but short-lived, chemodenervation (short survival time) or radiofrequency (long survival time) therapy is considered. Larger prospective, randomized, multicenter clinical trials are necessary to validate our outcomes and refine the role of CT guidance in multimodal pain management in this specific population.