Multimodal management strategies for chronic pain after spinal surgery: a comprehensive review
Article information

Abstract
“Chronic pain after spinal surgery” (CPSS) is a nonspecific term for cases in which the end result of surgery generally does not meet the preoperative expectations of the patient and surgeon. This term has replaced the previous term i.e., failed back surgery syndrome. CPSS is challenging for both patients and doctors. Despite advancements in surgical techniques and technologies, a subset of patients continue to experience persistent or recurrent pain postoperatively. This review provides an overview of the multimodal management for CPSS, ranging from conservative management to revision surgery. Drawing on recent research and clinical experience, we aimed to offer insights into the diverse strategies available to improve the quality of life of CPSS patients.
INTRODUCTION
Recently, as the frequency of spinal surgery has increased, the incidence of failed back surgery syndrome (FBSS), in which patients experience postoperative pain, has also increased.
The International Association for the Study of Pain (IASP) defines FBSS as "lumbar spinal pain of unknown origin either persisting despite surgical intervention or appearing after surgical intervention for spinal pain originally in the same topographical location” [1]. It is a non-specific term that generally refers to an event wherein the final outcome of surgery does not meet the preoperative expectations of patients and surgeons [2].
This refers to cases in which pain does not decrease but rather increases, or other complications occur after spinal surgery. Although it is a term that does not assume negligence on the part of the medical staff, the meaning of the word 'failed' It is associated with medical staff's negligence. To avoid this, FBSS was referred to with other terms that did not imply surgical failure, such as post-laminectomy syndrome, post-spine surgery syndrome, and post-lumbar surgery syndrome. The International Classification of Diseases (ICD)-11 published by the World Health Organization in June 2018 called FBSS “chronic pain after spinal surgery” (CPSS) [3]. In this review, we will refer to FBSS as CPSS in accordance with the ICD-11 classification.
CPSS is difficult to treat for spinal surgeons who perform surgery and pain physicians responsible for pain management. Since pain persists even after spinal surgery, patients with post-spinal surgery syndrome often distrust medical staff and treatments during their outpatient visits, hindering further treatment.
Therefore, physicians involved in pain management should identify the cause of pain and become familiar with the most suitable treatment for each situation in advance. Herein, we reviewed the overall aspects of CPSS and introduced treatments (including interventional procedures) That may be effective for pain management.
ETIOLOGY
A single cause for CPSS is difficult to determine. Pain typically results from a combination of factors. The etiological factors for CPSS have been divided into patient, operative, and postoperative factors (Table 1).
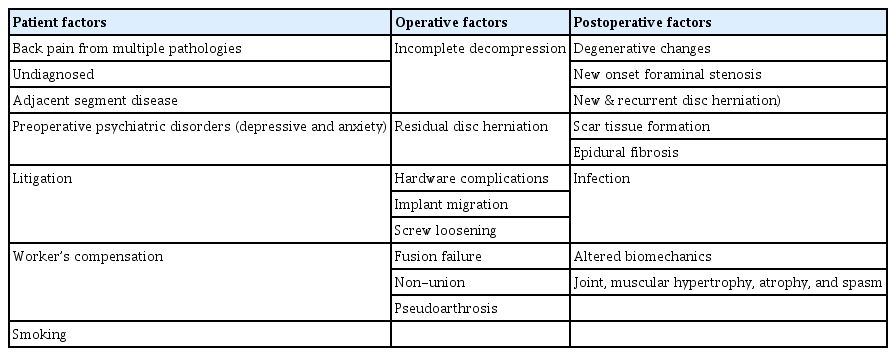
Summary of Factors Leading to Chronic Pain after Spinal Surgery
Patient factors
Appropriate surgery that meets the clinical conditions must be performed to achieve optimal outcomes in spinal surgery. If the chosen surgery is not suitable for a patient’s structural problems, there is a high probability that pain will persist postoperatively.
Undiagnosed or inadequately treated spinal stenosis at nonoperative levels can exacerbate pain and limit surgical success [4]. If the patient mainly shows axial back pain and undergoes decompression or intervertebral disc resection without fusion, the conducted surgery cannot be considered the most suitable for the patients’ clinical problem; thus, the pain will likely to continue postoperatively.
Preoperative magnetic resonance imaging (MRI) studies have shown that patients' psychosocial factors are more powerful than the structural abnormalities, and that patients' depression, anxiety disorders, somatization disorders, and health concerns have a negative impact on the prognosis of spinal surgery [5-7]. Therefore, it is more desirable to identify the psychosocial factors of the patient, prepare for proper preoperative treatment, actively implement postoperative pain education, and request cooperation from the Department of Psychiatry if necessary. It is important to accurately identify the psychosocial predisposition of patients before surgery and establish a treatment plan accordingly.
The economic impact of issues such as litigation or workers' compensation is also known to affect CPSS. These factors can create complex issues such as secondary gains, which may hinder patients’ motivation for pain improvement after surgery. Several studies have shown that financial compensation concerns inappropriately affect all outcomes, including postoperative pain severity, postoperative opioid use, postoperative functional improvement, and emotional stability [8-10]. Smoking is also associated with increased preoperative or postoperative complications such as impaired wound healing, increased infection rates, and increased spinal nonunion [11,12]. These results indicate that behavioral modification should also be recommended for successful surgery.
Operative factors
Spinal surgery includes surgery to improve lower extremity pain (e.g., decompression of a nerve root or intervertebral disc resection to treat spinal nerve symptoms) and surgery to improve axial back pain (e.g., fusion to treat intervertebral disc pain or instability) [13,14].
Common operative factors for CPSS include incomplete decompression, nerve damage, adjacent segment disease, and residual disc herniation. If the surgical procedure does not adequately relieve pressure on the nerves or remove the source of pain, patients may continue to experience symptoms [1].
CPSS also occurs when the effects of surgery on the motion segment are not fully considered. For example, suppose a patient with lower extremity pain has spinal stenosis and very weak spondylolisthesis, and if decompression is performed without fusion, spondylolisthesis progresses and progressive back pain develops in many cases. Suboptimal removal of compressive structures, such as herniated discs or bone spurs, can leave residual pressure on the neural structures, contributing to CPSS [15].
Hardware-related issues such as implant migration, screw loosening, irritation, and adjacent segment degeneration may necessitate revision surgery and contribute to CPSS [16]. Pain may also occur around the screw, causing chronic irritation of the surrounding soft tissue and bursa formation. Non-union or pseudarthrosis occurs when fusion surgery fails. Some non-union patients experience pain, but there are also patients who experience no pain [17]. Surgical alterations can increase stress on adjacent segments, leading to accelerated degeneration and CPSS [18]. If the nerve root is excessively pulled or damaged during surgery, pain may occur owing to abnormal nerve function after surgery. The larger the surgery with excessive incisions, the more severe the damage to muscles and ligaments, and the higher the possibility of adhesions around the nerves after surgery, which increases the likelihood of developing CPSS [19].
Postoperative factors
Even if the surgery is successful, the possibility of recurrence remains. The recurrence of foraminal stenosis or intervertebral disc herniation may be due to the worsening of an existing disease, incomplete surgery, or changes in the structures around the surgery [20]. Spinal fusion surgery can place additional stress on the adjacent vertebrae, leading to accelerated degeneration and pain in those segments [21]. In some cases, spondylolisthesis or spinal stenosis progresses rapidly due to increased dynamics in the adjacent segments above and below the surgical site. This can lead to spinal instability.
After spinal surgery, fibrous scar tissue can form around the surgical site, leading to compression or irritation of the nerves and this can result in pain and other neurological symptoms [22]. Epidural fibrosis results in the epidural space due to spinal surgery-related fibrosis is About 20–36% of all patients after spinal surgery experience pain due to epidural adhesion [23]. Some of the direct and indirect causes of pain are the pulling of spinal nerves due to epidural adhesion, ischemia, and obstruction of the flow of cerebrospinal fluid, which supplies nutrients around the nerves, [23]. However, fibrosis inevitably occurs in almost all patients during spinal surgery, and there has been an ongoing controversy as to whether this phenomenon is necessarily connected to pain and why each patient has a different prognosis [24].
Infections usually occur early but sometimes do not become apparent until weeks or months have passed. If accidental durotomy is not detected, it may lead to a pseudo-meningocele [25].
Altered biomechanics due to back surgery can result in increased tension in the prevertebral and postvertebral muscles that directly control the movement of the spine. Increased tension in these muscles can lead to stiffness, inflammation, spasms, and fatigue, all of which can cause pain in the paraspinal areas of the back [26].
ASSESSMENT
History taking
History taking is the most important part of evaluating CPSS patients. This is because it not only provides the information necessary to interpret other diagnostic factors but also serves as the basis for evaluation. Through history taking, pain physicians can gather essential information about a patients’ symptoms, medical history, and psychosocial factors [27]. The most important aspect of history-taking is to thoroughly describe the current pain, compare the pain before and after surgery, progress of pain recurrence over time, and pain responses to specific activities. It is also important to analyze whether the type of surgery performed on the patient is appropriate for the preoperative symptoms.
If the pain before and after surgery was almost the same in terms of severity, pain area, characteristics, and response to physical examination, then the problematic condition has not been corrected. This may be a diagnostic error, error of appropriate surgical selection, or incomplete surgery. However, if the symptoms change significantly, it is very likely that a new pathological condition has occurred, which could be a complication of surgery, technical failure, or progression of an underlying disease.
If back pain does not improve at all or recurs within days to months of surgery, it is highly likely that the pathology of the symptomatic structure was not properly resolved during the surgery, or the surgery could have been performed at the wrong level leading to complications, or an incorrect surgery was performed on a specific patient. If pain is partially relieved, it means that only some of the structural problems were corrected.
Similar to other common spinal diseases, the use of red and yellow flag concepts when evaluating CPSS patients can be an effective approach. Red flags are potential indicators of severe underlying conditions requiring immediate attention and further investigation. Identifying red flags can prevent potentially life-threatening or destructive situations from being overlooked through appropriate diagnostic testing and management. In contrast, yellow flags are psychosocial factors that can increase the risk of chronicity or disability in CPSS patients. Identifying and resolving yellow flags can guide appropriate referrals for psychological support and help manage overall pain. The typical red and yellow flags reported for CPSS are listed in Table 2 [28].
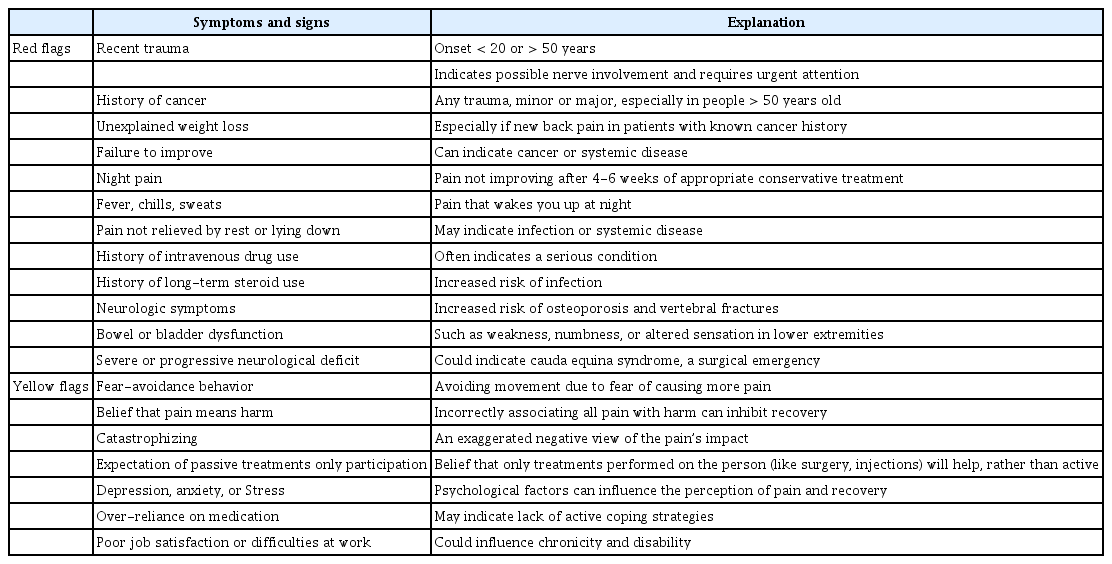
Identification of Red and Yellow Flags in Chronic Back Pain after Spinal Surgery
Imaging
Simple radiographs with an upright flexion/extension lateral view can determine the surgical location, arrangement of the spine, imbalance of the spine, instability, and degenerative changes. It can also be used to determine the degree of intervertebral space stenosis, anterior spondylosis, and pseudoarthrosis when fusion is performed [29].
Computed tomography (CT) can scan the surrounding area where spinal instruments are inserted more accurately than MRI can. Degenerative changes in the area adjacent to the surgical site, worsening of spondylolisthesis, and degenerative changes in the facet joint are easy to identify. CT myelogram can better reveal areas where spinal nerves are compressed by bony structures [30]. In addition, CT myelogram is a useful alternative because the presence of metallic implants can reduce the quality of images and the usefulness of diagnosis if the use of MRI is limited [31].
MRI is useful for detecting structural abnormalities such as herniated discs, fibrosis, infection, or hardware-related issues (e.g., screws or rods misplacement). It can also indicate a compression of the spinal nerves or nerve roots owing to disc protrusion or stenosis. Identifying nerve compression is crucial because it can explain the patients’ pain, and guide treatment decisions [32,33]. Information provided by MRI can help determine the appropriate course of treatment for CPSS patients, including further surgery, conservative management, or pain management techniques.
Technicium-99 single-photon emission computed tomography (SPECT) shows the anatomical sites of the radiotracer uptake, revealing enhancement of inflammatory areas, osteoblastic bone remodeling activity, and subtle segmental instability responsible for pain generation [34]. Various studies have investigated SPECT, identifying it as a promising technique for locating the foci of aseptic inflammation that serve as potential pain generators to help determine appropriate invasive or non-invasive treatment strategies [35]. It has therefore been proposed as a valuable tool for the localization of axial neck or back pain in patients who continue to experience unexplained CPSS [36].
Positron emission tomography (PET) can identify areas of inflammation, infection, or metabolic abnormalities in the spine [37]. PET is not routinely used for CPSS but can provide additional information when other imaging modalities yield inconclusive findings [38].
Diagnostic procedures
CPSS patients require examination because the facet joints and sacroiliac joints can cause pain [39]. Diagnostic articular injection is the standard method for diagnosing facet joint and sacroiliac joint syndrome [40]. CPSS may also result from disc herniation; in this case, a method of causing pain through lumbar discography is proposed [41]. It is important to determine the cause of lower extremity radiating pain in CPSS patients through physical examination and MRI to determine the area of spinal nerve compression. A transforaminal epidural block may be used to investigate whether nerves that appear compressed on MRI or CT are the pain-causing factors [42].
Epiduroscopy is the best minimally invasive method for visualizing the epidural space without damaging anatomical structures. It can be used to detect fibrosis, dissolve adhesions, and administer drugs to conventional fibrotic bands [43]. In CPSS patients, epiduroscopy can confirm epidural fibrosis and immediately confirm adhesion dissolution even if MRI reveals normal findings [44].
MANAGEMENT STRATEGIES
Persistent or recurrent pain associated with CPSS can severely impact a patient's quality of life, making it imperative to explore innovative pain management strategies beyond traditional approaches. Multimodal pain management, which combines various interventions, can be promising management strategy in the complex nature of CPSS.
Causative treatments
In CPSS patients, corrective treatments such as spinal stabilization, fusion, or decompression procedures, or interactive treatment are the rational first-line approach when the underlying cause for the associated pain is evident. for example, in surgical cases of inadequate decompression or fusion failure, intraoperative factors, inappropriate treatment, or also in non-surgical cases of pain.
Conservative managmenet
1. Physical therapy
Physical therapy plays a crucial role in the management of CPSS by improving mobility, strength, and overall function. It can also address musculoskeletal imbalances that contribute to pain [45]. Advanced physical therapy, including targeted exercises and stretching therapy can benefit CPSS patients because these methods address musculoskeletal imbalances, promote flexibility, and improving the overall function. These therapies should be individualized to patients’ specific condition and needs [46]. Chiropractic and osteopathic manipulations are alternative therapies that involve manual manipulation of the spine and musculoskeletal system. Although some CPSS patients may consider these therapies for pain relief or symptom management, they should be approached with caution. These treatments help relieve certain types of pain and improve functional abilities [47,48].
2. Pharmacological management
Before pharmacologically managing pain, it is important to understand the characteristics of pain (such as nociceptive or neuropathic pain) and its effects on daily life. Nociceptive pain is caused by tissue damage or inflammation and can be treated with nonsteroidal anti-inflammatory drugs (NSAIDs) [49]. If these are ineffective, non-opioid medications, such as high-dose NSAIDs, cyclo-oxygenase-2 (COX-2) inhibitors, or short-term corticosteroids can be introduced [50]. However, these drugs should be considered with caution because their long-term use can cause complications such as gastrointestinal bleeding, renal failure, and stroke. Opioid analgesics are not recommended for CPSS patients because the duration of prescription and the risks of long-term use are not clearly known; however, they can be used on a limited basis if used to improve short-term pain and function and to reduce the unwanted side effects of NSAIDs [51,52]. Muscle relaxants such as thiocolquicoside (a competitive gamma-aminobutyric acid (GABA) receptor antagonist) and tolperisone (a piperidine derivative and a centrally acting muscle relaxant) are good treatment options for patients with muscle spasm-related back pain [53].
Neuropathic pain caused by nerve damage or dysfunction can initially respond to antiepileptic drugs such as gabapentin and pregabalin, which are specifically designed to manage this type of pain [54]. Tricyclic antidepressants and selective norepinephrine reuptake inhibitors may also be effective for managing neuropathic pain [55].
Owing to the nature of the disease, it may be more effective to administer drugs with other mechanisms in combination rather compared to the effectiveness of single drugs. However, because all drugs have side effects on long-term use, the purpose behind pharmacotherapy is to increase the effectiveness of exercise and rehabilitation treatment rather than to achieve perfect pain control. Moreover, clinicians should select appropriate drugs and use it for only a minimum period of time.
3. Psychological support
Psychological therapies, such as cognitive-behavioral therapy [56], mindfulness-based stress reduction [57], pain education [58], and interdisciplinary pain rehabilitation [59], offer valuable tools to manage CPSS effectively. These therapies focus on addressing the psychological and emotional aspects of pain, enhancing coping strategies, and improving the overall quality of life for CPSS patients. However, individual differences in response to these therapies can occur, and a multidisciplinary approach involving consultation with a pain specialist is often recommended to tailor treatment to the patients’ specific needs.
Interventional pain procedure
1. Epidural blocks
Epidural blocks are the most common pain treatment worldwide. This procedure is primarily considered for patients experiencing pain after spinal surgery when conservative treatment is ineffective (Fig. 1). Epidural steroid injections can be used to diagnose and establish a treatment plan for CPSS by selecting an appropriate approach based on the patients’ symptoms [3].
(A) Anterior posterior view of caudal epidural block. (B) Lateral view of caudal epidural block. (C) Anterior posterior view of transforaminal epidural block at the left L5/S1 level. (D) Lateral view of transforaminal epidural block at the left L5/S1 level.
2. Facet joint procedures
In cases where facet joint pathology contributes to CPSS, corticosteroid or anesthetic injections into the affected joints can provide diagnostic and therapeutic benefits [60]. Radiofrequency ablation can be performed in anticipation of a 6-24 month reduction in pain if a diagnostic medial branch or facet joint block provides positive results in patients with CPSS caused by a facet joint (Fig. 2) [61].

(A) Anterior posterior view of lumbar medial branch block at the right L4 level. (B) Oblique view of facet joint block at the right L4/5 level.
3. Epidural adhesiolysis
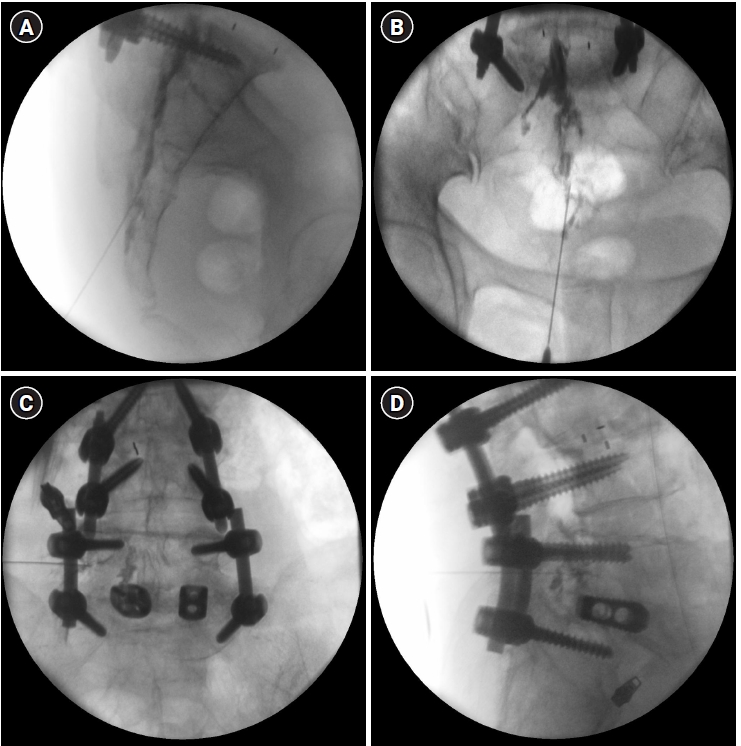
In any surgery, postoperative scar formation is a natural phenomenon during the tissue healing process. The same is true for the formation of epidural fibrotic adhesions after spinal surgery, but these adhesions may compress the nerve roots in 20-36% of patients, causing back or lower extremity pain [23]. Theoretically, adhesions can be lysed, thereby minimizing pain scores. Epidural adhesiolysis can be performed with hyaluronidase or hypertonic saline, and the combination of steroids and hyaluronidase may be more effective and last longer than either steroid alone [62]. Patients with epidural adhesions who are treated with hyaluronidase via a fluoroscopy-guided catheter can experience a significant decrease in pain score, disability index, and functional improvement (Fig. 3) [63]. Epidural adhesiolysis is more effective than epidural steroid injections [64].

Epidural adhesiolysis. (A) Epidural neuroplasty catheter was inserted into anterior epidural space. (B) Initial contrast was injected via the catheter. (C) Contrast reinjection after adhesiolysis demonstrating improved spread cephalad. (D) Lateral view of contrast spread.
The use of balloon expansion in the epidural space has also been recently introduced [65]. The method of including the balloon expansion function in the endoscopic catheter has the advantage of safely and effectively removing adhesions in a slightly wider area than that affected by the existing method because the balloon expansion function is included in the function of the existing catheter. However, more research is required for this.
Epiduroscopy makes it easy to remove adhesions while directly checking the area [66,67]. It achieves good long-term results in approximately 40% of CPSS patients who do not respond to other conventional treatments such as adhesiolysis with a Racz catheter [43,68]. A systematic review showed that pain and disability scores were clinically relevant 6-12 months after mechanical adhesiolysis in CPSS patients. The common complications associated with epiduroscopy include nerve injury, bleeding, infection, macular hemorrhage, and intracranial pressure [69,70].
4. Neuromodulation
Spinal cord stimulation (SCS) and intrathecal drug delivery systems (IDDS) have been shown to have promising effects in managing CPSS. These techniques can modulate pain signals and improve function [71,72]. SCS or IDDS can be used for refractory pain patients who do not respond to conventional treatment for CPSS. But, given the complications and management problems associated with after insertion, care should be taken when selecting this procedure.
Considerations for surgical revision
Revision surgery may be considered when the CPSS results from technical errors, inadequate decompression, or hardware-related issues. Careful patient selection and multidisciplinary teams are essential for successful outcomes [9]. However, revision surgery for CPSS has a low success rate and high morbidity risk. In patients who underwent instrumental fusion for CPSS treatment, only 35% reported a reduction in pain for approximately 15 months [73]. The absolute indications for revision surgery are the progression of neurological damage due to decreased functioning of organs or bladders, muscle weakness, and spinal nerve damage; and the relative indications are severe sciatica that persists or worsens despite 4 weeks of complete bed rest, recurrent episodes of incapacitating sciatica, pseudoarthrosis, abnormalities, or instability of surgical instruments [52].
CONCLUSION
CPSS is expected to occur continuously as long as spinal surgeries are performed. The greatest difficulty in its treatment is that patients are less responsive to conservative treatment, and nonsurgical treatment often does not result in satisfactory improvement. Multimodal pain management approaches represent a promising avenue for addressing the complex and debilitating nature of CPSS. Combining various methods, including pharmacological, interventional, physical, psychological, and complementary therapies allows for a holistic approach to pain relief. Although individual responses to these treatments vary, tailored multimodal approaches can significantly improve the quality of life for CPSS patients. Further research and personalized treatment plans are essential to optimize the outcomes in this challenging patient population.
Notes
FUNDING
None.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
AUTHOR CONTRIBUTIONS
Writing - original draft: Jung-Pil Yoon. Writing - review & editing: Hong-Sik Son, Jimin Lee, Gyeong-Jo Byeon. Conceptualization: Jung-Pil Yoon, Gyeong-Jo Byeon. Data curation: Hong-Sik Son, Jimin Lee. Methodology: Jung-Pil Yoon. Investigation: Jimin Lee, Gyeong-Jo Byeon. Resources: Jung-Pil Yoon. Software: Hong-Sik Son. Supervision: Gyeong-Jo Byeon. Validation: Gyeong-Jo Byeon.