


ņä£ļĪĀ
ņłśļ®┤ņĀ£ļéś ņĢäĒÄĖņ£Āņé¼ņĀ£ņÖĆ Ļ░ÖņØ┤ ņ×æņÜ®ņØ┤ ļ╣ĀļźĖ ņĢĮļ¼╝ņØś ņłśļ®┤ņŗ¼ļÅäņÖĆ ņ¦äĒåĄņŗ¼ļÅäļź╝ ņĀüņĀĢĒĢśļŖöļŹ░ ņé¼ņÜ®ļÉśļŖö ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģļ▓ĢņØĆ ņ▓┤ņżæ, ņŚ░ļĀ╣, ņĀ£ņ¦Ćļ░®ņ▓┤ņżæ(lean body mass) ļō▒ņØś ĒÖśņ×É ĒŖ╣ņØ┤ņĀü Ļ│Ąļ│Ćļ¤ē(covariate)Ļ│╝ ņ¦æļŗ©(population)ņØä ļīĆĒæ£ĒĢśļŖö ņé¼ļ×īņØś ņĢĮļÅÖĒĢÖ ļ¬©ņłśļź╝ ņłśĒĢÖņĀüņ£╝ļĪ£ ņŚ░Ļ▓░ņŗ£Ēé© ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬®Ēæ£ļåŹļÅäļź╝ ņØ╝ņĀĢĒĢśĻ▓ī ņ£Āņ¦ĆĒĢśļÅäļĪØ ņŻ╝ņ×ģņåŹļÅäļź╝ Ļ▓░ņĀĢĒĢśļŖö ļ░®ļ▓ĢņØ┤ļŗż[1,2]. PropofolņØä ņØ┤ņÜ®ĒĢ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģļ▓ĢņØĆ ņ¦äņĀĢĻ│╝ ļ¦łņĘ©ņŚÉ ļäÉļ”¼ ņé¼ņÜ®ļÉśļ®░, ņāüņÜ®ĒÖöļÉ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ņĀäņÜ®ĒÄīĒöäņŚÉļŖö ņłśņĀĢ Marsh ļ¬©ĒśĢĻ│╝ Schnider ļ¬©ĒśĢņØ┤ propofolņØś ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņ£╝ļĪ£ Ēāæņ×¼ļÉśņ¢┤ ņ׳ļŗż[3-5].
PropofolņØĆ ņżæņćäņżæņä▒ņ¦Ćļ░® propofol (medium chain triglyceride emulsion propofol, propofol-MCT/LCT), ņןņćäņżæņä▒ņ¦Ćļ░® propofol (long chain triglyceride emulsion propofol, propofol-LCT), ļ»ĖņäĖņ£ĀĒāüņĢĪ propofol (microemulsion propofol) ļō▒ ņŚ¼ļ¤¼ ņĀ£ĒśĢņØ┤ ņ׳ļŗż. ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ 5% soy-bean oil, 5% medium chain triglyceride, 1.2% purified yolk lecithin, 0.04% oleic acidļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ļŗż[6]. ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ 10% soy-bean oil, 2.25% glycerol, 1.2% egg phosphatideņØś ņ£ĀĒāüņĢĪ(emulsion)ņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ņ׳Ļ│Ā, ļ»ĖņäĖņ£ĀĒāüņĢĪ propofolņØĆ 10% purified poloxamer 188, 0.7% polyethylene glycol 660 hydroxystearate, 1% glycerin, 0.0008% disodium ethylenediaminetetraacetic acid (EDTA), 0.01% sodium ascorbateļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ļŗż[6,7]. ĻĘĖņżæņŚÉ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ ņ¦Ćņ¦ł Ļ┤ĆļĀ© ĒĢ®ļ│æņ”Ø, ņĀĢņŻ╝ĒåĄ ļ░Å ĒśłņĀäņĀĢļ¦źņŚ╝ņØś ļ░£ņāØņØ┤ ĒāĆ ņĀ£ĒśĢļ│┤ļŗż ļé«ņĢä ņé¼ņÜ®ņØ┤ ņ”ØĻ░ĆĒĢśņśĆļŗż[8].
ĒÖ£ņä▒ ļ¼╝ņ¦łņØĆ ļÅÖņØ╝ĒĢśļŹöļØ╝ļÅä ļŗżļźĖ ņĀ£ĒśĢņØś propofolņØĆ ļČĆĒśĢņĀ£ņŚÉ ļö░ļØ╝ ņĢĮļÅÖļĀźĒĢÖņĀü ĒŖ╣ņä▒ņØ┤ ļŗ¼ļØ╝ņ¦ł ņłś ņ׳ļŗż[9,10]. ļÅÖņØ╝ĒĢ£ ņ×ÉņøÉņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņןņćäņżæņä▒ņ¦Ćļ░® propofolĻ│╝ ļ»ĖņäĖņ£ĀĒāüņĢĪ propofolņØä ĻĄÉņ░©ņäżĻ│äļĪ£ ņ¦äĒ¢ēĒĢ£ ņĢĮļÅÖļĀźĒĢÖ ļ¬©ĒśĢĒÖö ņ×äņāüņŗ£ĒŚśņŚÉņä£, ļæÉ ņĀ£ĒśĢņØś ĒÖ£ņä▒ņä▒ļČäņØĆ 1% propofolļĪ£ ļÅÖņØ╝ĒĢśņśĆņ¦Ćļ¦ī, ņØ╝ļČĆ ņĢĮļÅÖĒĢÖ, ņĢĮļĀźĒĢÖ ļ¬©ņłśļŖö ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż. ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ ļ»ĖņäĖņ£ĀĒāüņĢĪ propofolļ│┤ļŗż ĒĢŁņĀĢņāüĒā£ ļČäĒżņÜ®ņĀüņØ┤ 50 L ņ╗ĖĻ│Ā, Ce50ņØĆ 0.4 ╬╝g/ml ļŹö ņ╗Ėļŗż[9]. ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉ ņØśĒĢśļ®┤ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolĻ│╝ ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ ņ£Āņé¼ĒĢ£ ņĢĮļÅÖļĀźĒĢÖ ĒŖ╣ņä▒ņØä ļ│┤ņśĆļŗż[11]. ļæÉ ņĀ£ĒśĢņØä ļ╣äĻĄÉĒĢśļŖö ļ¬®ņĀüņØś ņØ┤ ņŚ░ĻĄ¼ļŖö, ļ¦łņ¦Ćļ¦ē ņ▒äĒśł ņŗ£Ļ░äņØä ņČ®ļČäĒ׳ ĻĖĖĻ▓ī ņäżņĀĢĒĢśņ¦Ć ņĢŖņĢäņä£ ņĀ£Ļ▒░ĻĖ░(elimination phase)ļź╝ ļ░śņśüĒĢśņ¦Ć ļ¬╗ĒĢśņŚ¼ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolĻ│╝ ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØ┤ ņ▓┤ļé┤ņŚÉ ņĀĢņŻ╝ļÉśņŚłņØä ļĢī ļ│┤ņØ┤ļŖö ņĢĮļÅÖĒĢÖ ĒŖ╣ņä▒ņØä ņØ┤ĻĄ¼ĒÜŹ ņ£ĀņäĀļ¬©ĒśĢņ£╝ļĪ£ ņäżļ¬ģĒĢśļŖö ĒĢ£Ļ│äļź╝ Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż. ļö░ļØ╝ņä£ propofolņØś Ļ░ü ņĀ£ĒśĢņŚÉ ļ¦×ļŖö ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļéś, ņāüņÜ®ĒÖöļÉ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ĒÄīĒöäņŚÉļŖö ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņé¼ņÜ®ĒĢśņŚ¼ ĻĄ¼ņČĢļÉ£ ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢļ¦īņØ┤ Ēāæņ×¼ļÉśņ¢┤ ņ׳ņ£╝ļ»ĆļĪ£ ļČĆļōØņØ┤ĒĢśĻ▓ī ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņØ┤ļōż ļ¬©ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņĀĢņŻ╝ĒĢĀ ņłśļ░¢ņŚÉ ņŚåļŗż. ņØ┤ņĀä ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņØ┤ņÜ®ĒĢśņŚ¼ ĻĄ¼ņČĢĒĢ£ ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņ£╝ļĪ£ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ņŗ£Ē¢ēĒĢśņŚ¼ļÅä Ēü¼Ļ▓ī ļ¼ĖņĀ£Ļ░Ć ņŚåņØä Ļ▓āņ£╝ļĪ£ ņśłņāüņØĆ ļÉśņ¦Ćļ¦ī[11], ĻĘĖ ņĀĢĒÖĢņä▒ņŚÉ ļīĆĒĢ┤ņä£ļŖö ņŚ░ĻĄ¼ļÉ£ ļ░öĻ░Ć ņŚåļŗż.
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņżæņćäņżæņä▒ņ¦Ćļ░® propofol ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖźņØä ĒÅēĻ░ĆĒĢĀ ļĢī ņ¢╗ņØĆ ĻĖ░ņĪ┤ propofol ļåŹļÅä ņĖĪņĀĢņ×ÉļŻīņÖĆ propofol ņĀĢņŻ╝ ņØ┤ļĀź(infusion history) ņ×ÉļŻīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņłśņĀĢ Marsh ļ¬©ĒśĢ Ēś╣ņØĆ Schnider ļ¬©ĒśĢņŚÉņä£ņØś ĒśłņןļåŹļÅäļź╝ Ļ│äņé░ĒĢśņŚ¼ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ļ¬®Ēæ£ļåŹļÅä ņĪ░ņĀłņŻ╝ņ×ģĒĢĀ Ļ▓ĮņÜ░ TCI systemņØś ņśłņĖĪ ņä▒ļŖźņØä ĒÅēĻ░ĆĒĢśĻ│Āņ×É ĒĢ£ļŗż[12,13].
ļīĆņāü ļ░Å ļ░®ļ▓Ģ
ļ│Ė ņŚ░ĻĄ¼ļŖö ņżæņćäņżæņä▒ņ¦Ćļ░® propofol (Freefol, Daewon pharm, Korea) ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖźņØä ĒÅēĻ░ĆĒĢĀ ļĢī ņ¢╗ņØĆ propofol ļåŹļÅä ņĖĪņĀĢņ×ÉļŻīņÖĆ propofol ņĀĢņŻ╝ ņØ┤ļĀź ņ×ÉļŻīļź╝ ņĢäņé░ĒÄīĒöä ĒöäļĪ£ĻĘĖļש(version 2.1.3, Bionet Co., Ltd., Korea)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņŗ£ļ«¼ļĀłņØ┤ņģś ļČäņäØĒĢśņśĆļŗż. ņżæņćäņżæņä▒ņ¦Ćļ░® propofol ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖźņØä ĒÅēĻ░ĆĒĢĀ ļĢīļŖö ļ│Ė ĻĖ░Ļ┤Ć ņ×äņāüņŚ░ĻĄ¼ņŗ¼ņØśņ£äņøÉĒÜīņØś ņŖ╣ņØĖņØä ĒÜŹļōØĒĢ£ ĒøäņŚÉ ņ¦äĒ¢ēĒĢśņśĆĻ│Ā(ņŖ╣ņØĖļ▓łĒśĖ: 2016-0008), ļ│Ė ņŚ░ĻĄ¼ļź╝ ņ£äĒĢ┤ņä£ļŖö ņČöĻ░ĆņØś ņŖ╣ņØĖņØä ļ░øņ¦Ć ņĢŖņĢśļŗż. ņżæņćäņżæņä▒ņ¦Ćļ░® propofol ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖźņØä ĒÅēĻ░ĆĒĢ£ ņ×äņāüņŗ£ĒŚś ļé┤ņÜ®ņØä Ļ░äļץĒ׳ ņåīĻ░£ĒĢśļ®┤ ļ¦łņĘ© ņ£Āņ¦Ć ņŗ£ĻĖ░ņŚÉ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolļĪ£ ĻĄ¼ņČĢĒĢ£ ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņ£╝ļĪ£ ļ¬®Ēæ£ĒÜ©Ļ│╝ņ▓śļåŹļÅäļź╝ 2-6 ╬╝g/ml ļ▓öņ£ä ļé┤ņŚÉņä£ ļ│ĆĒÖöņŗ£ņ╝£ Ļ░Ćļ®┤ņä£ ņØ╝ņĀĢ ļåŹļÅäļź╝ 20ļČä ņØ┤ņāü ņ£Āņ¦Ćņŗ£Ēé© Ēøä ļÅÖļ¦źĒśł ņ▒äĒśłņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒÅēĻĘĀņĀüņ£╝ļĪ£ ĒĢ£ ĒÖśņ×ÉņŚÉĻ▓īņä£ 6ļ▓ł ņĀĢļÅäņØś ņ▒äĒśłņØ┤ ņØ┤ļŻ©ņ¢┤ņĪīļŗż. ņŚ¼ĻĖ░ņŚÉņä£ ĒÜŹļōØĒĢ£ Ļ░ü ĒÖśņ×ÉņØś ņŻ╝ņ×ģņØ┤ļĀź(infusion history)ņØś ņŗ£Ļ░äļ│ä Ēł¼ņŚ¼ļ¤ēĻ│╝ ņŻ╝ņ×ģņåŹļÅäļź╝ ņ×ģļĀźļ¤ēņ£╝ļĪ£ ĒĢśņŚ¼ ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņ£╝ļĪ£ ņĀĢņŻ╝ĒĢśņśĆņØä Ļ▓ĮņÜ░ Ļ░ü ņ▒äĒśł ņŗ£Ļ░äņŚÉ ļīĆĒĢ£ ņśłņĖĪĻ░ÆņØä ĻĄ¼ĒĢśņśĆļŗż. ņØ┤ ņśłņĖĪĻ░ÆĻ│╝ propofolņØś ĒśłņןļåŹļÅä ņĖĪņĀĢņ×ÉļŻīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolļĪ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ņŗ£Ē¢ēĒĢśņśĆņØä ļĢīņØś ņłśņĀĢ MarshņÖĆ Schnider ļ¬©ĒśĢņØś ņśłņĖĪ ņä▒ļŖźņØä ĒÅēĻ░ĆĒĢśņśĆļŗż[14]. ņśłņĖĪ ņłśĒ¢ēļÅä ĒÅēĻ░ĆļŖö Varvel ļō▒[15]ņŚÉ ņØśĒĢ┤ ņĀ£ņŗ£ļÉśņŚłļŹś ļ░®ļ▓ĢņŚÉ ļö░ļØ╝ ņĀäņ▓┤ ĒÖśņ×ÉĻĄ░ņŚÉ ļīĆĒĢ┤ ņłśĒ¢ē ņśżņ░© ļ░▒ļČäņ£©(performance error, PE)ņØä Ļ│äņé░ĒĢ£ Ēøä ņłśĒ¢ēņśżņ░©ņżæņĢÖĻ░Æ(median performance error, MDPE), ņłśĒ¢ēņśżņ░© ņĀłļīĆņżæņĢÖĻ░Æ(median absolute performance error, MDAPE), ļČäĻĖ░ļÅä(divergence)ņÖĆ ļÅÖņÜöļÅä(wobble)ļź╝ ĻĄ¼ĒĢśņśĆļŗż.
PEļŖö ļŗżņØīņØś ņŗØņŚÉ ļö░ļØ╝ Ļ│äņé░ĒĢśņśĆļŗż. iļ▓łņ¦Ė ĒÖśņ×ÉņŚÉņä£ jļ▓łņ¦Ė ĒśłņĢĪņØä ņ▒äņĘ©ĒĢĀ ļĢī ņŗżņĀ£ļĪ£ ņĖĪņĀĢĒĢ£ Ēśłņן propofolņØś ļåŹļÅäĻ░Ć CmijņØ┤Ļ│Ā, ņØ┤ ļĢīņØś propofolņØś ņĢĮļÅÖĒĢÖ ļ¬©ņłśņŚÉ ņØśĒĢ┤ ņśłņĖĪļÉ£ Ļ░ÆņØĆ CpijņØ┤ļŗż.
MDPEļŖö ņ╣śņÜ░ņ╣©(bias)ņØś ņĀĢļÅä, ņ”ē ņŗ£ņŖżĒģ£ņØś ĒÅēĻĘĀņĀüņØĖ overshoot Ēś╣ņØĆ undershootņØä ļ░śņśüĒĢśļ®░ ļŗżņØīņØś ņŗØņŚÉ ļö░ļØ╝ Ļ│äņé░ĒĢĀ ņłś ņ׳ļŗż.
MDAPEļŖö ņłśĒ¢ēļÅäņØś ļČĆņĀĢĒÖĢļÅä(inaccuracy)ļź╝ ņØśļ»ĖĒĢśļ®░, ņśłņĖĪ ņłśĒ¢ēļÅä ĒÅēĻ░ĆņŚÉ ņ׳ņ¢┤ Ļ░Ćņן ņżæņÜöņŗ£ ļÉśļŖö ņ▓ÖļÅäņØ┤ļ®░, ļŗżņØī ņŗØņŚÉ ņØśĒĢ┤ņä£ Ļ│äņé░ĒĢĀ ņłś ņ׳ļŗż.
ļČäĻĖ░ļÅäļŖö ņŗ£Ļ░äņŚÉ ļö░ļźĖ ņłśĒ¢ēļÅäņØś ļ│ĆĒÖöļź╝ ņĖĪņĀĢĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļŗżņØīĻ│╝ Ļ░ÖņØ┤ Ļ│äņé░ļÉ£ļŗż.
(tijļŖö ĒśłņĢĪņāśĒöī ijĻ░Ć ņ▒äņĘ©ļÉĀ ļĢīņØś ņŗ£Ļ░äņØä ņØśļ»ĖĒĢ£ļŗż)
ļÅÖņÜöļÅäļŖö ņłśĒ¢ēņśżņ░©ņŚÉņä£ ņĀäņ▓┤ņĀüņØĖ Ļ░£ņ▓┤ ļé┤ ļ│ĆņØ┤ļÅä(intra-individual variability)ļź╝ ņĖĪņĀĢĒĢśļŖö Ļ▓āņ£╝ļĪ£, ņØ┤ļŖö ņĢĮļ¼╝ ļåŹļÅäļź╝ ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆĒĢĀ ņłś ņ׳ļŖö ĻĖ░ļŖźĻ│╝ ņ¦üņĀæ Ļ┤ĆļĀ©ļÉ£ļŗż.
ņĀäņ▓┤ ĒÖśņ×ÉĻĄ░ņŚÉ ļīĆĒĢ£ ĒÅēĻ░ĆļŖö Varvel ļō▒[15]ņŚÉ ņØśĒĢ┤ ņåīĻ░£ļÉ£ pooled data approachļź╝ ļö░ļ×Éļŗż.
Ļ▓░Ļ│╝
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö, ņØ┤ņĀä ņżæņćäņżæņä▒ņ¦Ćļ░® propofol ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖź ĒÅēĻ░ĆņŚÉ ņ░ĖņŚ¼ĒĢ£ 35ļ¬ģņØś ĒÖśņ×ÉņŚÉĻ▓īņä£ ņ¢╗ņØĆ 217Ļ░£ņØś propofol ļåŹļÅä ņĖĪņĀĢĻ░ÆņØä ņØ┤ņÜ®ĒĢśņśĆļŗż. ņżæņćäņżæņä▒ņ¦Ćļ░® propofol ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪņä▒ļŖź ĒÅēĻ░ĆņŚÉ ņ░ĖņŚ¼ĒĢ£ 35ļ¬ģ ĒÖśņ×ÉņØś ĒŖ╣ņä▒ņØä Table 1ņŚÉ ņĀ£ņŗ£ĒĢśņśĆļŗż. PropofolņØś ĒśłņןļåŹļÅä ņĖĪņĀĢĻ░ÆĻ│╝ ņØ┤ņŚÉ ļīĆņØæĒĢśļŖö ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņŚÉņä£ņØś ļåŹļÅä ņśłņĖĪĻ░ÆņØś Ļ┤ĆĻ│äļź╝ Fig. 1ņŚÉ ļéśĒāĆļé┤ņŚłļŗż. ņØ╝ņ╣śņäĀ(line of identity)ņØś ┬▒ 30% ļ▓öņ£ä ļ░¢ņŚÉ ņØ╝ļČĆ ņ×ÉļŻīļōżņØ┤ ļČäĒżĒĢśņśĆļŗż. Fig. 2ņŚÉņä£ļŖö Ļ░ü ĒÖśņ×ÉņØś ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņŚÉņä£ņØś ļåŹļÅä ņĖĪņĀĢĻ░ÆņŚÉ ļīĆĒĢ£ ļåŹļÅä ņśłņĖĪĻ░ÆņØś ļ╣äņ£©ņØä ņŗ£Ļ░äņŚÉ ļö░ļźĖ ļ│ĆĒÖöļĪ£ Ēæ£ņŗ£ĒĢśņśĆļŗż. ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢ©ņŚÉ ļö░ļØ╝ ņśłņĖĪĻ░ÆĻ│╝ ņĖĪņĀĢĻ░ÆņØś ļ╣äĻ░Ć ĒŖ╣ņĀĢĒĢ£ Ļ▓ĮĒ¢źņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. Pooled data approachņŚÉ ņØśĒĢ┤ ņŗ£Ē¢ēĒĢ£ ļæÉ ļ¬©ĒśĢņØś ņśłņĖĪ ņłśĒ¢ēļÅä ņ¦æļŗ© ļČäņäØ Ļ▓░Ļ│╝ļŖö Table 2ņŚÉ ņĀ£ņŗ£ĒĢśņśĆļŗż. Schnider ļ¬©ĒśĢņŚÉņä£ inaccuracy, ņ”ē MDAPE Ļ░ÆņØĆ 26.3%ļĪ£ Varvel ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśņśĆņ¦Ćļ¦ī ņ£ĀņØśĒĢ£ ĒÄĖĒ¢źņØä ļ│┤ņśĆļŗż. ņłśņĀĢ Marsh ļ¬©ĒśĢņØś Ļ▓ĮņÜ░ MDAPE Ļ░ÆņØ┤ 30%ļź╝ ņ┤łĻ│╝ĒĢśņśĆņ¦Ćļ¦ī, Schnider ļ¬©ĒśĢņØś MDAPEņÖĆ ņŗżņĀ£Ļ░Æ Ļ░äņØś ņ░©ņØ┤ļŖö Ēü¼ņ¦Ć ņĢŖņĢśļŗż.
Table┬Ā1
Characteristics of Patients (n = 35)
| ŌĆāAge (yr) | ŌĆā53 (47.8-57.8)ŌĆā |
| ŌĆāWeight (kg) | 68.4 ┬▒ 12.7 |
| ŌĆāHeight (cm) | 166.8 ┬▒ 8.7 |
| ŌĆāLBM (kg) | 50.5 ┬▒ 10.0 |
| ŌĆāMale/FemaleŌĆā | 26/9 |
| ŌĆāASA PS 1/2 | 14/21 |
Data are presented as counts, mean ┬▒ SD, or median (25-75%), as appropriate. LBM: lean body mass calculated using Janmahasatian formula [22]. ASA PS: American Society of Anesthesiologists physical status
Fig.┬Ā1
Measured vs. estimated plasma concentration of propofol for the modified Marsh model (A) and Schnider model (B). The red solid line represents the line of identity; that is, the estimated concentration is equal to the measured concentration. The dashed lines represent a bias of ┬▒ 30%.

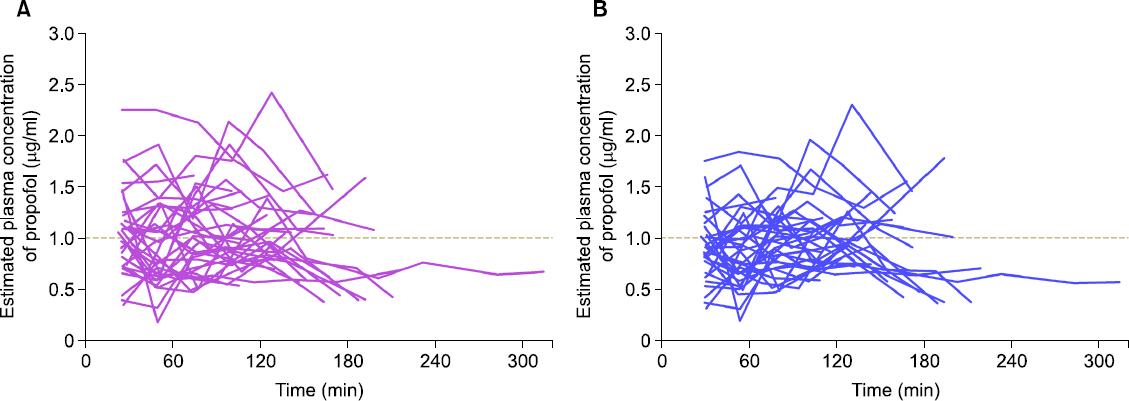
Fig.┬Ā2
The estimated-to-measured propofol concentration ratio over time for the modified Marsh model (A) and Schnider model (B). A ratio of 1 means that measured concentration equals estimated concentration.
Table┬Ā2
Pooled Biases, Inaccuracies, Divergences, and Wobbles of the Modified Marsh and Schnider Models
Ļ│Āņ░░
PropofolņØĆ ņĀĢļ¦ź Ēł¼ņŚ¼ņŚÉ ņĀüĒĢ®ĒĢśņ¦Ć ņĢŖņØĆ ļČłņłśņÜ®ņä▒ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ļŗżļźĖ ļČĆĒśĢņĀ£ņÖĆ Ļ▓░ĒĢ®ĒĢ£ ļŗżņ¢æĒĢ£ ņĀ£ĒśĢņØ┤ Ļ░£ļ░£ļÉśņŚłļŗż[6]. ļČĆĒśĢņĀ£ļōżņØĆ ņĀĢņŻ╝ĒåĄ, ļ»ĖņāØļ¼╝ ņ”ØņŗØ, ņ¦Ćņ¦łĻ┤ĆļĀ© ĒĢ®ļ│æņ”Ø ļō▒ņØś ņøÉņØĖņØ┤ ļÉ£ļŗż[8]. ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØĆ ņןņćäņżæņä▒ņ¦Ćļ░® propofolņŚÉ ļ╣äĒĢ┤ ņżæļō▒ļÅä ņØ┤ņāüņØś ņĀĢņŻ╝ĒåĄņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā[8,16], ņןņćäņżæņä▒ņ¦Ćļ░® propofolņØä Ēł¼ņŚ¼ĒĢĀ ļĢī ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö Ļ│Āņżæņä▒ņ¦Ćļ░®Ēśłņ”Ø, ņĘīņןņŚ╝Ļ│╝ Ļ░ÖņØĆ ņ¦Ćņ¦ł Ļ┤ĆļĀ© ĒĢ®ļ│æņ”ØņØä Ļ░Éņåīņŗ£Ēé©ļŗż[17,18]. ņØ┤ļ¤¼ĒĢ£ ņןņĀÉņŚÉ ĻĘ╝Ļ▒░ĒĢśņŚ¼ ņ×äņāüņĀüņ£╝ļĪ£ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØś ņé¼ņÜ®ņØ┤ ņ”ØĻ░ĆĒĢśņśĆļŗż.
ĒÜ©Ļ│╝ņĀüņØĖ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ņ£äĒĢ┤ņä£ļŖö ņé¼ņÜ®ņ×ÉĻ░Ć ņäżņĀĢĒĢ£ ļ¬®Ēæ£ Ēśłņן ļåŹļÅäņŚÉ ĻĘ╝ņĀæĒĢśĻ▓ī ņŗżņĀ£ ņĢĮļ¼╝ņØś ĒśłņןļåŹļÅäĻ░Ć ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ļČĆņĀĢĒÖĢņä▒(inaccuracy)ņØä ņĖĪņĀĢĒĢśļŖö ņ▓ÖļÅäņØĖ ņłśĒ¢ēņśżņ░©ņĀłļīĆņżæņĢÖĻ░Æ(MDAPE)ņØĆ ņśłņĖĪ ņłśĒ¢ēļÅä ĒÅēĻ░ĆņŚÉņä£ Ļ░Ćņן ņżæņÜöĒĢ£ ņ¦ĆĒæ£ļĪ£, ĻĘĖ Ļ░ÆņØ┤ 20-30% ļ»Ėļ¦īņØ╝ ļĢī ĒĢ┤ļŗ╣ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ņŗ£ņŖżĒģ£(TCI system)ņØĆ ņ×äņāüņĀüņ£╝ļĪ£ ņé¼ņÜ®ņØ┤ Ļ░ĆļŖźĒĢśļŗż[12,19]. ņØ┤ļ▓ł ņŚ░ĻĄ¼ņŚÉņä£ ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņØś MDAPEļŖö Ļ░üĻ░ü 32.1%, 26.3%ļĪ£, ļæÉ ļ¬©ĒśĢņØ┤ ņ×äņāüņĀüņ£╝ļĪ£ ĒŚłņÜ® Ļ░ĆļŖźĒĢ£ ņłśņżĆņØä ļ│┤ņśĆļŗż. ņłśņĀĢ Marsh ļ¬©ĒśĢņŚÉņä£ļŖö ņłśĒ¢ēņśżņ░©ņżæņĢÖĻ░Æ(MDPE)ņØś 95% ņŗĀļó░ĻĄ¼Ļ░äņŚÉ 0ņØä ĒżĒĢ©ĒĢśņŚ¼ ņ£ĀņØśĒĢ£ ĒÄĖĒ¢źņØĆ ņŚåņŚłņ¦Ćļ¦ī, Schnider ļ¬©ĒśĢņŚÉņä£ļŖö 0ņØä ĒżĒĢ©ĒĢśņ¦Ć ņĢŖņĢä Ļ│╝ļīĆņśłņĖĪ(overprediction)ĒĢśļŖö ņ£ĀņØśĒĢ£ ĒÄĖĒ¢źņØä ļ│┤ņśĆļŗż. ļČäĻĖ░ļÅäņØś Ļ▓ĮņÜ░ ĻĘĖ Ļ░ÆņØ┤ 0ņŚÉ ĻĘ╝ņĀæĒĢĀ ņĀĢļÅäļĪ£ ņ×æņØĆ Ļ▓āņØ┤ ļ░öļ×īņ¦üĒĢśļ®░, ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļČäĻĖ░ļÅä ŌłÆ2.4%/h, 0%/hļĪ£ ļæÉ ļ¬©ĒśĢ ļ¬©ļæÉ ņŗ£Ļ░äņØś ĒØÉļ”äņŚÉ ļö░ļźĖ ņśłņĖĪ ņłśĒ¢ēļÅäņØś ļ│ĆĒÖöĻ░Ć ņĀüņŚłļŗż. ļÅÖņÜöļÅäļŖö ļæÉ ļ¬©ĒśĢņŚÉņä£ Ļ░üĻ░ü 15.4%, 12.8%ņśĆņ£╝ļ®░, ņØ┤ļŖö ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņŚÉņä£ ņĢĮļ¼╝ļåŹļÅäļź╝ ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆĒĢĀ ņłś ņ׳ņØī ņØśļ»ĖĒĢ£ļŗż. TCI systemņØś ņśłņĖĪņä▒ļŖźņØ┤ ņóŗņØäņłśļĪØ ņØ╝ņ╣śņäĀņØä ņżæņŗ¼ņ£╝ļĪ£ ņśłņĖĪĻ░ÆņØ┤ ļ░Ćņ¦æĒĢśĻ▓ī ļÉśĻ│Ā, ņØ╝ņ╣śņäĀņØś ┬▒ 30% ļ▓öņ£ä ļ░¢ņŚÉ ņ£äņ╣śĒĢśļŖö ņśłņĖĪĻ░ÆļÅä Ļ▒░ņØś ņŚåĻ▓ī ļÉ£ļŗż. ņØ┤ņ▓śļ¤╝ ņĖĪņĀĢĻ░ÆĻ│╝ ņśłņĖĪĻ░ÆņØś Ļ┤ĆĻ│äļź╝ ĻĘĖļ”╝ņ£╝ļĪ£ ĻĘĖļĀżļ│┤ļ®┤ ņĀäļ░śņĀüņØĖ ņä▒ļŖźņØä ņ¦üĻ┤ĆņĀüņ£╝ļĪ£ Ļ░ĆļŖĀĒĢ┤ ļ│╝ ņłś ņ׳ļŗż. TCI systemņØś ņśłņĖĪņä▒ļŖźņØ┤ ņóŗņØäņłśļĪØ ņśłņĖĪĻ░ÆĻ│╝ ņĖĪņĀĢĻ░ÆņØś ļ╣äĻ░Ć 1ņŚÉ Ļ░ĆĻ╣īņÜ┤ Ļ░ÆņØä Ļ░Ćņ¦ĆĻ▓ī ļÉśļ®░, ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢ©ņŚÉ ļö░ļØ╝ņä£ļÅä 1 ņŻ╝ņ£äļĪ£ Ļ░ÆņØ┤ ļéśĒāĆļéśĻ▓ī ļÉĀ Ļ▓āņØ┤ļŗż. ļ¦īņØ╝ ņŗ£Ļ░äņØ┤ Ļ▓ĮĻ│╝ĒĢ©ņŚÉ ļö░ļØ╝ ņśłņĖĪĻ░ÆĻ│╝ ņĖĪņĀĢĻ░ÆņØś ļ╣äĻ░Ć ņĀÉņ░© ņ”ØĻ░ĆĒĢśĻ▒░ļéś Ēś╣ņØĆ Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņØ╝ Ļ▓ĮņÜ░ ņØ┤ļŖö TCI systemņØś ļČĆņĀĢĒÖĢļÅäļź╝ ļ░śņśüĒĢ┤ ņżĆļŗżĻ│Ā ļ│╝ ņłś ņ׳ļŗż.
Glen ļō▒[12,14]ņØ┤ ņ×äņāüņŚÉņä£ ņé¼ņÜ®ļÉśļŖö ņןņćäņżæņä▒ņ¦Ćļ░® propofol ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ļ¬©ĒśĢņŚÉ ļö░ļźĖ ņśłņĖĪ ņłśĒ¢ēļÅäļź╝ ĒÅēĻ░ĆĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņØś MDAPEĻ░Ć Ļ░üĻ░ü 24-26%, 20-23% ļ▓öņ£äņŚÉņä£ ņé░ņČ£ļÉśņŚłĻ│Ā, ņØ┤ļ▓ł ņŗ£ļ«¼ļĀłņØ┤ņģś ļČäņäØņŚÉņä£ ļæÉ ļ¬©ĒśĢņØś MDAPEļŖö ļ¬©ļæÉ ņØ┤ņĀä ņŚ░ĻĄ¼ņÖĆ ņ£Āņé¼ĒĢśņśĆļŗż. ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ĒĢĀ ļĢī Ēśłņן ļåŹļÅäļź╝ ņØ╝ņĀĢĒĢśĻ▓ī ņ£Āņ¦ĆĒĢśĻĖ░ ņ£äĒĢ£ ņ¦ĆņåŹ ņĀĢņŻ╝ ņåŹļÅäļŖö ļŗżņØī ņŗØņ£╝ļĪ£ Ļ│äņé░ĒĢ£ļŗż[20].
ņŚ¼ĻĖ░ņŚÉņä£ ņŗ£Ļ░äņØ┤ ļ¼┤ĒĢ£ļīĆļĪ£ Ļ░äļŗżĻ│Ā Ļ░ĆņĀĢņØä ĒĢśļ®┤, ņĀĢņŻ╝ ņåŹļÅäļŖö ļŗżņØī ņŗØņ£╝ļĪ£ Ēæ£ĒśäļÉ£ļŗż.
ņ”ē, ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņŚÉņä£ ņ¦ĆņåŹ ņĀĢņŻ╝ ņåŹļÅäļź╝ Ļ▓░ņĀĢĒĢśļŖöļŹ░ ņżæņÜöĒĢ£ ņĢĮļÅÖĒĢÖ ļ¬©ņłśļŖö ņ▓Łņåīņ£©(clearance)ņØ┤ļŗż. ņä£ļĪ£ ļŗżļźĖ ņĀ£ĒśĢņØś propofolņØĆ ĒÖ£ņä▒ ļ¼╝ņ¦łņØĆ ļÅÖņØ╝ĒĢśļ»ĆļĪ£ ņ▓Łņåīņ£©ņØ┤ ņ£Āņé¼ĒĢĀ Ļ▓āņØ┤ļ®░, ļæÉ ņĀ£ĒśĢ ņé¼ņØ┤ņŚÉ MDAPEĻ░ÆļÅä ņ£Āņé¼ĒĢĀ Ļ▓āņØ┤ļŗż. ņןņćäņżæņä▒ņ¦Ćļ░® propofolĻ│╝ ļ»ĖņäĖņ£ĀĒāüņĢĪ propofolņØś ņĢĮļÅÖļĀźĒĢÖņĀü ĒŖ╣ņä▒ņŚÉ ļīĆĒĢ£ ņØ┤ņĀä ņŚ░ĻĄ¼ņŚÉņä£, ļæÉ ņĀ£ĒśĢ Ļ░ä ņ▓Łņåīņ£©(clearance)ņØĆ 1.55 L/min, 1.53 L/minņ£╝ļĪ£ ņ£Āņé¼ĒĢśņśĆĻ│Ā[9], ņןņćäņżæņä▒ņ¦Ćļ░®Ļ│╝ ņżæņćĀņżæņä▒ņ¦Ćļ░® ĒöäļĪ£ĒżĒÅ┤ņØś ņĢĮļÅÖļĀźĒĢÖ ĒŖ╣ņä▒ņØä ļ╣äĻĄÉĒĢ£ ņØ┤ņĀä 1ņāü ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ▓Łņåīņ£©ņØĆ ļÅÖņØ╝ĒĢśņśĆļŗż[11]. ļö░ļØ╝ņä£ ņØ┤ļōż ņĀ£ĒśĢņØś ņĢĮļÅÖĒĢÖņĀü ņ░©ņØ┤ļŖö ļČĆĒśĢņĀ£ņŚÉ ņØśĒĢ£ ļČäĒż(distribution)ņ░©ņØ┤ņŚÉ ĻĖ░ņØĖĒĢśņśĆņØä Ļ▓āņØ┤ļŗż.
ņØ┤ļ▓ł ņŚ░ĻĄ¼ņØś ņĀ£ĒĢ£ņĀÉņØĆ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ņØ┤ļĀź ņ×ÉļŻīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņŗ£Ē¢ēĒĢ£ ņŗ£ļ«¼ļĀłņØ┤ņģś ņŚ░ĻĄ¼ļĪ£, ņŗżņĀ£ļĪ£ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņé¼ņÜ®ĒĢśņŚ¼ ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņ£╝ļĪ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ĒĢśļ®░ propofol ļåŹļÅäļź╝ ņŗżņĖĪĒĢśņ¦Ć ņĢŖņĢśļŗżļŖö ņĀÉņØ┤ļŗż. ĒĢśņ¦Ćļ¦ī Glen and Servin [12]ņØś propofolņØś ļäż Ļ░Ćņ¦Ć ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪ ņłśĒ¢ēļÅäļź╝ ĒÅēĻ░ĆĒĢ£ ņŚ░ĻĄ¼, Absalom ļō▒[21]ņØ┤ ketamineņØś ņäĖ Ļ░Ćņ¦Ć ņĢĮļÅÖĒĢÖ ļ¬©ĒśĢņØś ņśłņĖĪ ņłśĒ¢ēļÅäļź╝ ĒÅēĻ░ĆĒĢ£ ņŚ░ĻĄ¼ ļō▒ņŚÉņä£ļÅä ņŗ£ļ«¼ļĀłņØ┤ņģśņØ┤ ņé¼ņÜ®ĒĢśņŚ¼ ņŗ£Ē¢ēļÉśņŚłĻ│Ā, ņØ┤ ĻĖ░ļ▓ĢņØĆ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņ×ÉļŻīļź╝ ĒÖ£ņÜ®ĒĢśņŚ¼ ļ¬©ĒśĢņØś ņśłņĖĪ ņä▒ļŖźņØä ĒÅēĻ░ĆĒĢśļŖö ļ░®ļ▓Ģņ£╝ļĪ£ ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£, ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ņŗ£Ē¢ēĒĢśņśĆņØä Ļ▓ĮņÜ░ Schnider ļ¬©ĒśĢņØĆ Varvel ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśņśĆņ¦Ćļ¦ī ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ ĒÄĖĒ¢źņØä ļ│┤ņØĖ ļ░śļ®┤, ņłśņĀĢ Marsh ļ¬©ĒśĢņØś Ļ▓ĮņÜ░ MDAPEĻ░Ć 30%ļź╝ ļ▓Śņ¢┤ļé¼ņ¦Ćļ¦ī Schnider ļ¬©ĒśĢņØś MDAPEņÖĆ ņŗżņĀ£Ļ░ÆņŚÉņä£ļŖö Ēü░ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņ£ĀņØśĒĢ£ ĒÄĖĒ¢źļÅä ņŚåņŚłļŗż. ļö░ļØ╝ņä£ Ēśäņ×¼ ņāüņÜ®ĒÖöļÉ£ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģ ĒÄīĒöäļź╝ ņé¼ņÜ®ĒĢśņŚ¼ ņżæņćäņżæņä▒ņ¦Ćļ░® propofolņØä ņłśņĀĢ Marsh, Schnider ļ¬©ĒśĢņ£╝ļĪ£ ļ¬®Ēæ£ĒÜ©Ļ│╝ņ▓śļåŹļÅä ņĪ░ņĀł ņŻ╝ņ×ģļ▓ĢņØä ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØ┤ Ļ░ĆļŖźĒĢśļŗż. ņČöĻ░ĆļĪ£ ļæÉ ņĀ£ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬®Ēæ£ļåŹļÅäņĪ░ņĀłņŻ╝ņ×ģņØä ĒĢśņśĆņØä Ļ▓ĮņÜ░ ņØśņŗØņåīņŗżņŗ£Ļ░ä, Ļ░üņä▒ņŗ£Ļ░äņØä ļ╣äļĪ»ĒĢ£ ņĢĮļĀźĒĢÖņĀü ņ×äņāüņ¦ĆĒæ£ļōżņØä ļ╣äĻĄÉĒĢśļŖö ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒĢĀ ĒĢäņÜöņä▒ņØ┤ ņ׳ļŗż.




