A comparative study of glottis visualization according to the method of lifting the epiglottis in video laryngoscopy: indirect and direct lifting methods
Article information

Abstract
Background
The direct entry of the camera under the epiglottis may provide a better view of the glottis than the indirect lifting of the epiglottis by placing the Macintosh blade tip on the vallecula when using the video laryngoscope. This study aimed to compare the efficiency of two different methods of lifting the epiglottis during the visualization of glottis using video laryngoscopy in the same patient.
Methods
This prospective study enrolled 60 patients who underwent general anesthesia with tracheal intubation. In each patient, glottic views were obtained by directly (group DE) and indirectly lifting the epiglottis (group IE). These two methods were compared using the modified Cormack and Lehane grade and the percentage of glottis opening (POGO) score as assessment parameters.
Results
Modified Cormack and Lehane grade showed a significant difference between the groups DE and IE (P = 0.004). The difference in the POGO score between the groups DE and IE was also statistically significant (87.5% and 64.4%, respectively; P < 0.001).
Conclusions
Our results, therefore, revealed that the method of directly lifting epiglottis was better at exposing glottis than the method of indirectly lifting epiglottis using a video laryngoscope.
INTRODUCTION
Tracheal intubation, in which an appropriate endotracheal tube is inserted into the trachea through the oral or nasal cavity to secure the airway, is the most important routine practice for anesthesiologists. During the process of tracheal intubation, it is imperative to overcome the anatomical characteristics presented by the angled airway to ensure a line of sight to the glottis. To achieve this, direct laryngoscopes (DLs) are commonly used for the alignment of the oral, pharyngeal, and laryngeal axes, and for the elevation of the epiglottis. Among the methods that employ DLs, despite the enormous progress in anesthetic practice, exposing the glottis by indirect elevation of epiglottis using a Macintosh blade (Macintosh method) developed by RR Macintosh in 1943 [1] is still the most used method worldwide.
Recently, the method of intubation has changed from that involving a direct glottic view to an indirect glottic view because video laryngoscopes (VL) have several advantages such as improvement of glottis visualization, a higher intubation success rate, reduction in intubation attempts and complications compared to direct laryngoscopes [2–10]. The VL that uses an indirect glottis view can confirm the location of the glottis on an external monitor via a camera located in the middle or tip of the blade. Even when the direct laryngoscopy cannot directly identify the laryngeal structures such as epiglottis through the oral cavity, the video laryngoscopy can observe the laryngeal structures because of the camera position in the pharynx. Most of the manufacturers of VLs recommend the Macintosh method to lift epiglottis indirectly. However, considering that VL uses the indirect glottic view of the camera close to the glottis, the method of exposing the glottis by lifting the epiglottis directly may be more appropriate.
Thus, we hypothesized that the direct entry of the camera under the epiglottis may provide a better glottic view than the indirect lifting of the epiglottis by placing the blade tip in the vallecula in the VL. We compared the indirect and direct methods of lifting the epiglottis for visualization of glottis using VL in the same patient.
MATERIALS AND METHODS
This study was conducted as a prospective study after approval from the Institutional Review Board (IRB no. 2020-04-015) and included 60 patients. This study was registered at ClinicalTrials.gov (no. KCT0005170). All patients were recruited from a single medical center. All the patients enrolled were over 18 years of age and had American Society of Anesthesiologists physical status 1–2. These patients were scheduled for general anesthesia with tracheal intubation. All the patients provided written informed consent to the study. The patients with cardiovascular or respiratory diseases, risk of aspiration, history of difficult intubation, and poor dental conditions were excluded from this study.
Method
Non-invasive blood pressure, electrocardiogram, pulse oximetry, bispectral index, and monitoring of neuromuscular blocking with train of four (TOF ratio) were performed as standard monitoring in all patients. Glycopyrrolate (0.2 mg) was administered intravenously before induction of anesthesia. General anesthesia was induced with 1–2 mg/kg propofol, 0.8 mg/kg rocuronium, and remifentanil (target-controlled infusion). When “zero” TOF count was recorded twice continuously after the administration of a neuromuscular blocking agent, the glottic view was obtained by two methods of lifting the epiglottis directly and indirectly using VL (AceScope, Acemedical Co., Korea) with a curved blade (single use). The blade of the VL was inserted along the midline of the tongue, and the shape and location of the epiglottis was confirmed. First, for the direct method, the blade was placed under the epiglottis and lifted to expose the glottis. Second, for the indirect method, the blade was pulled back and the tip of the blade was placed on the tongue base (vallecula) and lifted epiglottis indirectly to expose the glottis. In order to minimize the harm to the patient, both methods were performed in a sequential process. No external laryngeal manipulation was performed. The best glottic view was taken for each method, and intubation was performed using a stylet during the indirect method. In the direct method, attempts to enter the blade under the epiglottis were limited to three. The video laryngoscopy was performed by an experienced anesthesiologist (more than 5 years of experience as an anesthesiologist). The results of the video laryngoscopy were divided into two groups based on the method used for the exposure of glottis; the group in which the epiglottis was lifted directly (group DE) and the group in which the epiglottis was lifted indirectly (group IE). The glottic view was compared in the two groups using the captured images.
Measurement
Patient’s demographic data was collected, and airway assessment including Mallampati class, mouth opening, thyromental distance, and neck mobility was performed. The primary outcome of video laryngoscopy was the modified Cormack and Lehane (CL) grade of the glottic view (grade 1; full view of the glottis, grade 2a; partial view of the glottis, grade 2b; arytenoids or posterior part of the vocal cords only just visible, grade 3; only epiglottis visible, grade 4; neither glottis nor epiglottis visible) [11]. Laryngoscopy grading was performed by an anesthesiologist who did not perform video laryngoscopy. The secondary outcome was the percentage of glottis opening (POGO) score [12] and adverse events such as severe bradycardia or asystole, and laryngospasm were recorded. The landmark of POGO was the anterior commissure (anterior) and interarytenoid notch (posterior). POGO score was based on the subjectivity of the estimator, and measured on a scale of 0–100% in steps of 10%. The scoring was performed by three anesthesiologists, and the mean of the assigned scores were used.
Study sample size and statistical analysis
When the pilot study (n = 26) was conducted, the difference in incidence of modified CL grade 1 in the two groups (direct elevation group: 96.2%, indirect elevation group: 69.2%) was 27%. When the sample size was calculated at an α level of 0.05 and a power of 0.8 based on this result of the pilot study, each group was estimated to have 54 cases. It was decided to include 60 cases in each group (total 120 cases) by adding 10% of cases to compensate for dropout rates. Since each procedure was performed serially on the same patient, the study was conducted in a total of 60 patients. Statistical analysis was performed using SPSS ver. 23 (IBM Co., USA) Patient demographic and airway assessment data are expressed as mean (95% confidence interval). The two methods were performed sequentially in same patient, but because each method was independent, modified CL grade was analyzed using the chi-squared test and POGO score was analyzed using the t-test. A P value < 0.05 was considered to be statistically significant.
RESULTS
The demographic and airway assessment data of the patients are as shown in Table 1. Modified CL grade showed significant difference between group DE and group IE (P = 0.004). The difference in the POGO scores between group DE and group IE was also statistically significant (87.5% and 64.4, %respectively; P < 0.001). The superiority of glottic view (Fig. 1) by POGO score in the same patient was 43 (71.7%) and 8 (13.3%) in group DE and group IE, respectively (Table 2). There were no cases where the blade failed to enter under the epiglottis in the group DE. In addition, there were no cases of laryngospasm or cardiac arrhythmias related to laryngoscopy.

Patients Demographic and Airway Assessment Data
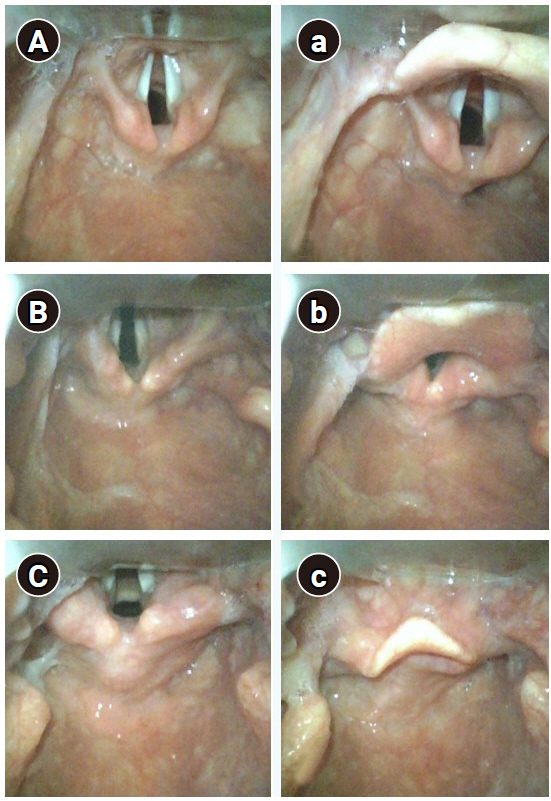
Paired glottic view in the same patient (A-a, B-b, C-c). The capital letter is a method of lifting the epiglottis directly, and the small letter is a method of lifting the epiglottis indirectly in the same patient. The glottic view obtained by lifting the epiglottis directly shows superiority.

Glottis Visualization
DISCUSSION
In this study, we assessed the efficacy of two different methods of lifting the epiglottis (direct and indirect) for visualization of the glottis in the same patient using VL. Our results revealed that the method of directly lifting the epiglottis was better at exposing the glottis than the method of indirectly lifting epiglottis using a VL. In addition, upon evaluation of the glottic view using each of the two methods on the same patient, we observed that most cases using the direct method showed superior glottic view.
The VL developed for difficult airway management in the early 2000s combines the advantages of DLs and fiberoptic bronchoscopes [2–4]. VL uses a blade as in a direct laryngoscope. However, VL uses an indirect glottic view that helps to identify the glottis on an external monitor through a camera located on the blade. In direct laryngoscopy using direct glottis view, the two steps including the alignment of the three airway axes and the elevation of the epiglottis by direct or indirect method, should be performed simultaneously to expose the glottis. For epiglottis elevation, the Macintosh laryngoscope is most commonly used as an indirect method of applying force on the vallecula (tongue base). This method is significantly affected by the anatomical variety of the epiglottis such as size, shape, rigidity, and the relationship with connected structures such as hyoid bone and hyoepiglottic ligament [13]. In contrast, because the camera in the VL is located in the pharynx, the alignment of the airway axes is not important. Therefore, it is most important to raise the epiglottis, which is the final barrier concealing the glottis from the camera’s view. Even though the VL and Macintosh laryngoscope are fundamentally different in the methods used to approach the glottis, the Macintosh method is recommended mainly for most of the VLs. When the Macintosh method is also used in video laryngoscope for epiglottis elevation, the hindrance offered by laryngeal anatomy cannot be avoided. However, the camera of VL can easily enter the posterior aspect of the epiglottis, and this method is, therefore, considered to be less affected by the anatomy of the larynx.
Macintosh method, developed in 1943, has been used as a standard method for tracheal intubation for decades, and although VLs are popularly used, this is still used as the gold standard in evaluating other devices [14,15]. Most of the VL studies compared glottis visualization, intubation success rate at overall and/or the first attempt, time to intubation, and complication, with those observed using the Macintosh laryngoscope. In many studies, VL has been reported to improve glottis visualization, increase intubation success rate, reduce intubation attempts, reduce pressure on laryngeal structures, and reduce complications compared to those observed on using the Macintosh laryngoscope [3–9,16]. Since the VL is evolving rapidly and has various advantages over Macintosh laryngoscope, it is considered that VL will become a routine practice in airway management during anesthesia in place of the Macintosh laryngoscope in the near future. It is important to conduct further investigations to determine the most appropriate method for using VL. Similar to this study, these investigations should address the followings: glottis visualization using VL, whether to use the stylet when entering the endotracheal tube or how to properly form the stylet, and the usefulness of the channel on the blade.
The limitation of this study is that the study related to intubation according to each method could not be conducted as both methods were performed simultaneously in the same patient. In addition, because the superiority of glottis visualization does not indicate the superiority in intubation, further investigations related to intubation that involve the intubation success rate, time to intubation, and complications in each method will be needed.
In conclusion, our results demonstrated that when exposing the glottis using a VL, the method of directly lifting the epiglottis provided a superior glottic view than the indirect method.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
DATA AVAILABILITY
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
AUTHOR CONTRIBUTIONS
Conceptualization: Yu Yil Kim. Data curation: Ji Youn Oh, Seung Min Baek, Da Wa Jung, Ji Hun Park. Writing - original draft: Yu Yil Kim. Writing - review & editing: Yu Yil Kim. Supervision: Ji Hye Lee.