Postoperative pain control by ultrasound guided brachial plexus block reduces emergence delirium in pediatric patients
Article information

Abstract
Background:
Pediatric patients awakening from general anesthesia may experience emergence delirium (ED), often due to inadequate pain control. Nerve block completely inhibits innervation of the surgical site and is superior to systemic analgesics. This study assessed whether pain control through nerve block relieves ED after general anesthesia.
Methods:
Fifty patients aged 2–7 years with humerus condyle fractures were randomly assigned to receive ultrasound guided supraclavicular brachial plexus block (BPB group) or intravenous fentanyl (Opioid group). The primary outcome was score on the pediatric anesthesia emergence delirium (PAED) scale on arrival at the postanesthesia care unit (PACU). Secondary outcomes were severity of agitation and pain in the PACU, the incidence of ED, and postoperative administration of rescue analgesics over 24 h.
Results:
PAED scale was significantly lower in the BPB group at arrival in the PACU (7.2 ± 4.9 vs. 11.6 ± 3.2; mean difference [95% confidence interval (CI)] = 4.4 [2.0–6.8], P < 0.001) and at all other time points. The rate of ED was significantly lower in the BPB group (36% vs. 72%; relative risk [95% CI] = 0.438 [0.219–0.876], P = 0.023). The BPB group also had significantly lower pain scores and requiring rescue analgesics than Opioid group in the PACU.
Conclusions:
Ultrasound guided BPB, which is a good option for postoperative acute phase pain control, also contributes to reducing the severity and incidence of ED.
INTRODUCTION
Emergence delirium (ED) in pediatric patients is defined as a ‘dissociated state of consciousness, in which the child is irritable, uncompromising, uncooperative, incoherent, and inconsolably crying, moaning, kicking, or thrashing’ [1]. ED occurs mainly in children aged 2–5 years [2], lasts for 5–30 min and is self-limiting. However, active treatment and management are necessary to prevent self-inflicted injury, contamination of the surgical site, and removal of intravenous (IV) catheters or drains [3]. ED may also be associated with post-operative separation anxiety and behavioral disturbances such as sleep and eating disorders [4].
The risk factors for ED include rapid emergence from anesthesia, short acting volatile agents, type of surgery, age, preoperative anxiety, and postoperative pain [1]. Pain is not the sole cause of ED, but post-operative pain is thought to increase the risk of ED. Fentanyl is widely used to control pain and ED in children [5,6]. However, in an effective pain control dose of fentanyl, inevitable complications occur such as nausea, vomiting, respiratory depression and unwanted deep sedation.
The Pediatric Regional Anesthesia Network has shown that regional anesthesia in pediatric patients performed while under general anesthesia and while awake, is safe and effective for acute postoperative pain control [7,8]. Ultrasonography, in particular, allows peripheral nerve block to be safely performed in pediatric patients, leading to increases in the numbers of children administered regional anesthesia [9,10].
Although regional anesthesia techniques can help control acute postoperative pain, their ability to reduce ED rates remains unclear. This prospective randomized study evaluated whether active pain control by ultrasound-guided brachial plexus block (BPB) can effectively reduce ED after pediatric orthopedic surgery. We hypothesized that BPB would reduce the severity and incidence of ED.
MATERIALS AND METHODS
This parallel, randomized controlled, observer-blinded, study was performed from June 2016 to June 2017. The study protocol was approved by the institutional ethics committee of our hospital (no. 2016-05-036-001) and was prospectively registered at the Clinical Research Information Service, a clinical trial registry in Korea (KCT0002086). The parents or legal guardians of all included patients provided written informed consent.
Inclusion criteria were patients scheduled to undergo surgery for humerus condyle fractures, aged 2–7 years, and American Society of Anesthesiologists physical status I. Patients were excluded if they had multiple injuries, local infection, mental retardation, hypersensitive to amide anesthetics such as ropivacaine, their parents or guardians refused consent.
The primary outcome was score on the pediatric anesthesia emergence delirium (PAED) scale on arrival at the post anesthesia care unit (PACU) [11]. Secondary outcomes were scores on the PAED scale and the modified Children’s Hospital of Eastern Ontario Pain (mCHEOP) scale (Table 1) [11,12] measured at 5-min intervals in the PACU, the incidence of ED and administration time of rescue analgesics. The ED defined PAED scale on arrival at the PACU > 10.

All operations were performed under general anesthesia by a single surgeon (H.D.S.), this surgeon did not enter the operating room during induction of anesthesia and BPB administration. All patients underwent intravenous access in the ward and were premedicated with glycopyrrolate 0.04 mg/kg 30 min before induction of anesthesia. While the caregiver is with the patient in the preoperative area, ketamine 1.5 mg/kg was injected, following which the patient was moved to the operating room.
After the patient arrived in the operating room, an electrocardiograph, pulse oximeter, and noninvasive blood pressure monitor were attached, and vital signs were measured. Anesthesia was induced with 3 vol% of sevoflurane inhalation and rocuronium 0.6 mg/kg. Following tracheal intubation with a proper sized endotracheal tube, sevoflurane was adjusted within 2–3 vol% to maintain blood pressure and heart rate within 20% of baseline. Mechanical ventilation was set to maintain end tidal carbon dioxide at about 35 mmHg.
After induction of general anesthesia, enrolled patients were randomly assigned 1 : 1 to the BPB or Opioid group. To conceal group allocation, a computer-generated random number table with four blocks was uploaded into Redcap (web based data management program; http://redcap.cnuh.co.kr/) and used for randomization.
Groups were allocated by researchers conducting intervention and excluded from outcome measurements. The patients and caregivers, including the nurse who scored patients in the PACU, were blinded to group assignments by covering the real and predicted block needle insertion site with small sized dressings. Immediately after induction of general anesthesia, patients in the BPB group were administered 0.2% ropivacaine (0.5 ml/kg) under ultrasound guidance using a supraclavicular approach (i.e., into the intersection between the first rib and the subclavian artery) with MylabTM25 Gold (Esaote, Italy) and a linear probe (LA435: 6–18 MHz, Esaote). Aspiration was repeated in 0.5 ml increments. Patients in the Opioid group were administered 1 μg/kg of IV fentanyl at 2–3 min before incision or pinning, 0.5 μg/kg of IV fentanyl at 5 min before the end of surgery. All interventions in both groups were performed by a single skilled anesthesiologist. The block was deemed successful if, at the time the arm was tractioned or pinned to start surgery, the heart rate had not changed more than 20%.
After surgery, the neuromuscular block was reversed with pyridostigmine 0.2 mg/kg and glycopyrrolate 4 μg/kg, and the patient was extubated. The patient was transported to the recovery room when appropriate breathing and spontaneous eye opening were observed.
During the stay in the PACU, one nurse trained and experienced with the PAED and mCHEOP scales recorded these scores every 5 min. Rescue analgesics were administered to patients who exhibited a mCHEOP scale ≥ 5 or at the request of the parents. Rescue analgesics were IV fentanyl (0.5 μg/kg) in the PACU (postoperative 0–1 h) and IV paracetamol (15 mg/kg) in the ward (postoperative 1–24 h). Frequency of rescue analgesic administration and first request time were recorded. Postoperative complications including fever, nausea, vomiting, and any intervention related complication were noted.
The number of patients per group was calculated from results of other study showing that fascia iliaca block reduced mean PAED scale from 10.4 ± 3.2 to 7.3 ± 2.9 [13]. Using a two tailed. α = 0.05 and a power of 90%, a minimum sample size of 22 patients per group was calculated. Allowing for a 10% dropout rate, it was planned to recruit a total of 50 patients.
Statistical analyses were performed using R software version 3.4.2 (R Project for Statistical Computing, Austria). All analyses were performed by the intention to treat (ITT), which included patients with protocol violations. Additionally, we also proceeded with as treated analysis to evaluate the impact of protocol violations. The normality of continuous data was assessed using the Shapiro–Wilk test. If normality was satisfied, comparisons between groups were determined by independent t-tests, with the results expressed as mean ± SD. If normality was not satisfied, groups were compared using the Mann–Whitney U test, with the results expressed as median (interquartile range). Categorical data were compared using the chi-squared test or Fisher’s exact test, as appropriate. Survival outcomes, including time-to-event outcomes and median analgesia times, were analyzed by the Kaplan–Meier method and compared by the log-rank test. For all calculations, a two-tailed P value < 0.05 was considered statistically significant.
RESULTS
Of the 50 patients assessed for eligibility, none was excluded. These patients were randomly assigned 1 : 1 to one of the two groups. After random allocation two patients were found to be in violation of the protocol. After receiving the assigned intervention, two patients in the BPB group received intravenous fentanyl before emergence. These patients were included in ITT analysis. The statistically significant results did not change even if as treated analysis proceeded after excluding two patients. The Consolidated Standards of Reporting Trials (CONSORT) flow diagram is shown in Fig. 1, and the demographic and clinical characteristics of the two groups shown in Table 2. There was no complication in both groups. All patients in BPB group were judged to have successful BPB.
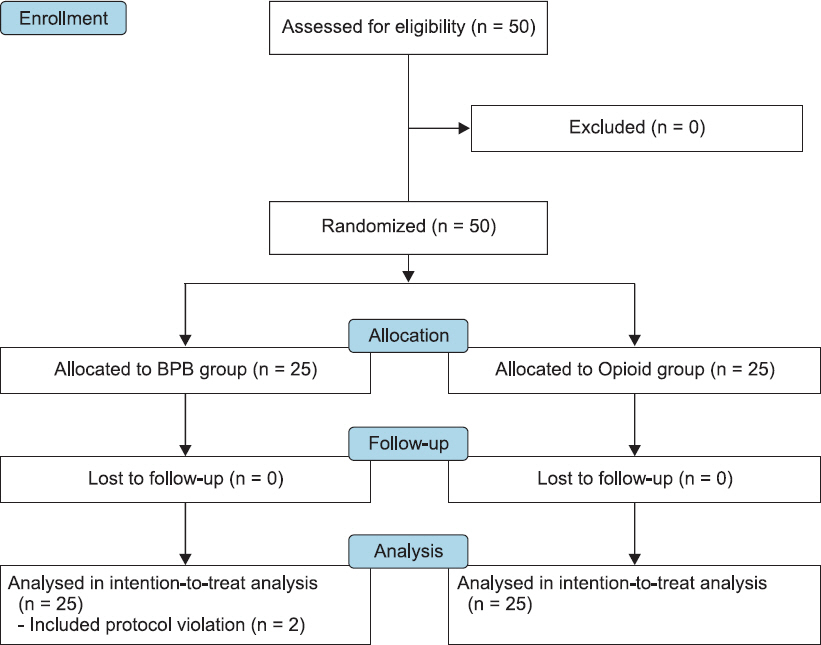
Consolidated Standards of Reporting Trials flow diagram of study participants. BPB: brachial plexus block.

Demographic and Clinical Characteristics of Patients in the Both Groups
The primary outcome, PAED scale at arrival in the PACU, was significantly lower in the BPB group than in the Opioid group (7.2 ± 4.9 vs. 11.6 ± 3.2; mean difference between groups = 4.4; 95% confidence interval [95% CI], 2.0–6.8, P < 0.001). The PAED scale was significantly lower in the BPB than in the Opioid group at all time points (Fig. 2A). The ED rate was also significantly lower in the BPB than in the Opioid group (36% [9/25] vs. 72% [18/25], relative risk = 0.438; 95% CI, 0.219–0.876, P = 0.023).
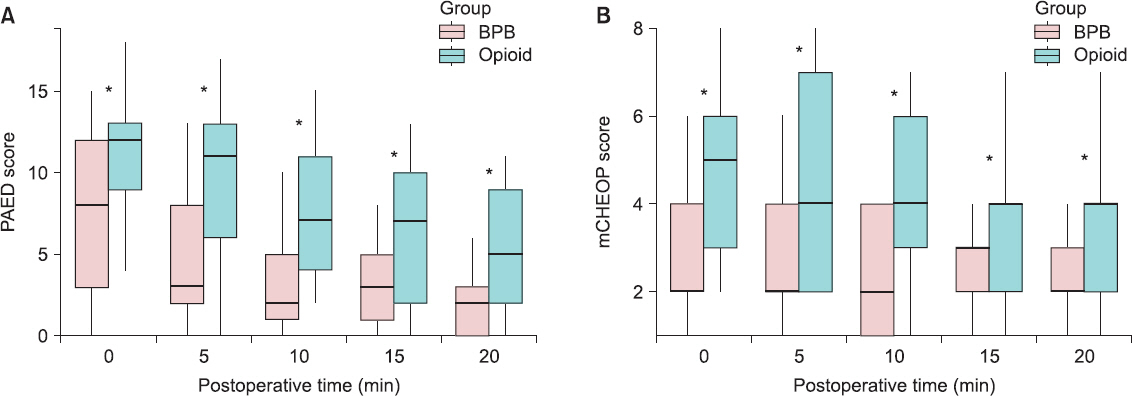
Scores over time of patients in the brachial plexus block (BPB) and Opioid groups assessed using (A) the pediatric agitation and emergence delirium (PAED) scale and (B) the modified Children's Hospital of Eastern Ontario Pain (mCHEOP) scale. Values are presented as median (1Q, 3Q). *P < 0.05 between two groups.
The mCHEOP scale were significantly lower in the BPB than in the Opioid group at all time points (Fig. 2B). The number of patients requiring rescue analgesics in the PACU was significantly lower in the BPB than in the Opioid group (2 [8%] vs.12 [48%], P = 0.005), but the number of patients requiring rescue analgesics in the ward did not differ (Table 3). The Kaplan–Meier survival analysis showed that the time to first rescue analgesic request was significantly longer in the BPB than in the Opioid group (7 vs. 2 h; hazard ratio = 2.01; 95% CI, 1.01–4.02, P = 0.048; Fig. 3).

Postoperative Outcomes of Patients in the BPB and Opioid Groups

Kaplan–Meier survival analysis showing the proportion of patients in the brachial plexus block (BPB) and Opioid groups not requiring rescue analgesics over time, with comparison by the log-rank test.
DISCUSSION
This study investigated the effect of postoperative pain control by nerve block on ED in pediatric patients. The results showed that, compared with IV fentanyl, ultrasound guided BPB reduces ED severity and incidence.
Risk factors for ED in pediatric patients include rapid emergence from anesthesia, use of short-acting volatile anesthetic agents, type of surgery, age, preoperative anxiety, and child temperament [1]. There is controversy as to whether pain is a risk factor for ED. The patients with postoperative agitation manifested as paranoia had no postoperative pain when recovered to a normal state [14]. Also, ED can occurs in pediatric patients undergoing non-painful exam like magnetic resonance imaging [15]. Although pain is not the sole cause of ED, surgery associated with severe postoperative pain is thought to increase the risk of ED. Preoperative analgesia was effective in reducing the risk of ED, presumably by delaying emergence and reducing postoperative pain [16]. Postoperative pain control using regional analgesia, such as caudal block, has been associated with ED rates of 20–30% [17,18]. In agreement with studies using regional analgesia [13], the present study found that the incidence of ED in the BPB group were about 36%. These results indicating that complete neural blockade does not completely prevent occurrence of ED due to other factors, but incidence of ED significantly reduced.
It is difficult to completely distinguish ED from paininduced behavior by PAED scale. Although PAED scale is known to be a representative and useful tool for ED diagnosis, the last two item on the PAED scale (restlessness and inconsolability) may reflect pain. Thus, delirium specific first three items on the PAED scale (eye contact, purposeful actions, awareness of surroundings) highly correlated with ED [17].
Prophylactic analgesia with fentanyl has been shown to reduce postoperative pain and ED [19,20]. Fentanyl is routinely administered perioperatively to pediatric patients undergoing surgery. Fentanyl acts as an agonist that binds to μ and k opioid receptors and has analgesic, sedative, and anesthetic properties. Fentanyl has a rapid onset of action of 2–3 min, a short duration of action of 60 min following bolus doses and minimal hemodynamic effects [21]. It is widely used to provide rapid short-lived pain relief during surgery. In our study, the opioid group receiving fentanyl was utilized as the active comparator group. The 0.5 μg/kg of fentanyl was administered at 2–3 min prior to incision, and at 5 min before the end of surgery. According to the recently published guideline of European Society for Paediatric Anaesthesiology [22], the intraoperative and postoperative fentanyl dose used in our study seems to be an adequate dose. Decreasing ED is more effective with high dose of fentanyl, but the risk of PONV increases [5].
Supraclavicular BPB can be used as a sole anesthetic method in arm fracture surgery [23]. However, BPB is usually administered after sedation or general anesthesia because pediatric patients tend to be uncooperative. Nerve blocks can be safely performed in pediatric populations undergoing general anesthesia or sedation because they do not increase the postoperative rates of neurologic symptoms or the toxicity of local anesthetics [7,8]. In pediatric patients, ultrasound guided BPB increases block success rates and improves block quality, as evaluated by block onset, duration and opioid consumption, making BPB excellent for post-operative pain control [9,24]. Indeed, we found that BPB significantly reduced analgesic requirements in the recovery room and significantly prolonged time to first dose of analgesic. In the recovery room two patients in the BPB group and 12 in the Opioid group required additional analgesics, with median times to first dose of BPB being 7 h, the duration of action of ropivacaine. Although BPB is effective in controlling acute pain, we observed no difference in the frequency of analgesics required over the first 24 h postoperative, which may have been due to the small sample size.
Most studies have used PAED cut-offs of 10 or 12 in ED diagnosis [17,25,26]. We have defined 10 as the cut off value, but even with the more strict value of 12, we found that BPB lowered the incidence of ED. Although the PAED scale was used to measure emergence agitation, no consensus has been reached regarding an appropriate cut-off value on this scale [11,25]. In the studies that analyzed the diagnostic value of PAED scale because the definition of ED was based on the clinical experience of one expert, it should be interpreted with caution. The diagnosis of ED in pediatric patients is complicated by the diversity of assessment tools, different definition of ED and the absence of a gold standard for diagnosis of ED.
This study had several limitations. Fisrt, there was a possibility that maintenance sevoflurane concentration may be lower in the BPB group. This may have resulted in less emergence agitation in this group [27,28]. The BPB was performed before the operation resulted in the suppression of intraoperative pain. Also, anesthesia depth was not controlled based on electroencephalography like BIS™ (Aspect Medical Systems, USA) [29], and sevoflurane concentration was not recorded. Second, we did not assess preoperative anxiety, which has been reported to promote and exacerbate ED. However, all children were given ketamine under parental supervision prior to surgery to minimize preoperative anxiety. Finally, the patients received both interventions were included in the ITT analysis. The results of the ITT might be more significant but the results of as treated analysis were similar. Therefore, according to CONSORT guidelines [30], all participants included in the analysis regardless of adherence to the protocol.
In conclusion, ultrasound guided BPB, which is a good option for postoperative acute phase pain control, also contributes to reducing the severity and incidence of ED. Based on our results, we think that postoperative pain contributes to the development of ED.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
ORCID
Boohwi Hong: https://orcid.org/0000-0003-2468-9271
Choonho Jung: https://orcid.org/0000-0001-5065-3374
Yumin Jo: https://orcid.org/0000-0002-4847-0250
Sookyoung Youn: https://orcid.org/0000-0002-8461-0599
Yeojung Kim: https://orcid.org/0000-0002-2079-670X
Woosuk Chung: https://orcid.org/0000-0002-6409-2325
Seok-Hwa Yoon: https://orcid.org/0000-0001-9344-6754
Hyun Dae Shin: https://orcid.org/0000-0003-4290-1125